Saccular Coronary Artery Aneurysm and Fistula with Organized Thrombi
- Affiliations
-
- 1Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. bjjake.kim@samsung.com
- 2Department of Cardiovascular and Thoracic Surgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Cardiovascular and Thoracic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1769650
- DOI: http://doi.org/10.4070/kcj.2013.43.2.127
Abstract
- Saccular coronary artery aneurysm, associated with coronary artery fistula, is a very rare condition. A 48-year-old woman was referred to our hospital for the evaluation of an abnormal shadow on the left cardiac border from a chest X-ray film during regular medical health examination. A huge saccular aneurysm with organized thrombi in the proximal left anterior descending artery (LAD) and coronary artery fistulae from LAD and conus branch of the right coronary artery to pulmonary artery was diagnosed by transthoracic echocardiography, multi-detector computer tomography (MDCT), and coronary angiography. The patient received surgical treatment, including thrombectomy of aneurysm, ligation of the inlet and outlet of aneurysmal sac, coronary artery bypass graft (left internal mammary artery-to-distal LAD), and ligation of fistulae. The postoperative course was uneventful, and postoperative echocardiography and MDCT revealed patent bypass graft; however, a small fistula from proximal LAD across aneurysmal sac to pulmonary artery was observed.
MeSH Terms
Figure
-
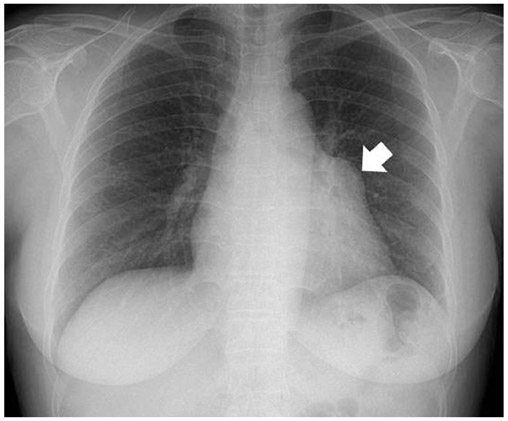
Fig. 1 The chest radiography of the patient shows abnormal heart shadow (arrow).
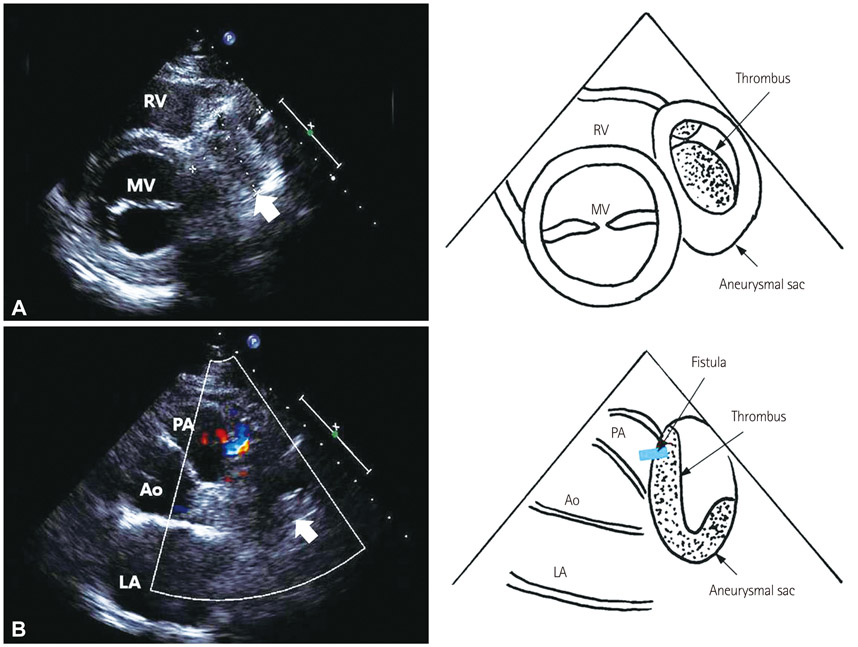
Fig. 2 The parasternal short axis view of transthoracic echocardiography. A: aneurysmal sac (arrow) filled with thrombus, size about 4.1×4.0 cm. B: fistula from aneurysmal sac to pulmonary the artery (color flow) and aneurysmal sac (arrow). Ao: aorta, LA: left atrium, MV: mitral valve, PA: pulmonary artery, RV: right ventricle.
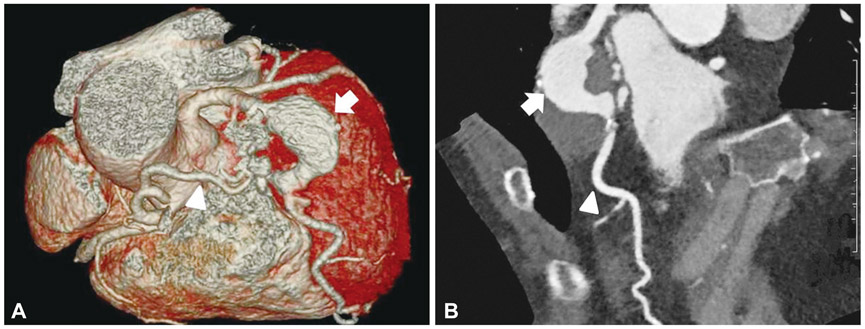
Fig. 3 Multi-detector computed tomography of the coronary artery. A: reconstructed image shows saccular aneurysm (arrow) of LAD with fistula (arrowhead) from the conus artery to pulmonary artery. B: LAD (arrowhead) and aneurysmal sac (arrow). LAD: left anterior descending artery.

Fig. 4 Coronary angiography. A: right coronary artery (arrowhead) and a fistula (arrow) from the conus artery to pulmonary artery (short thin aorrw). B: left anterior descending artery (arrowhead), aneurysmal sac (arrow), fistula (long thin arrow) from proximal LAD to pulmonary artery (short thin arrow). LAD: left anterior descending artery.
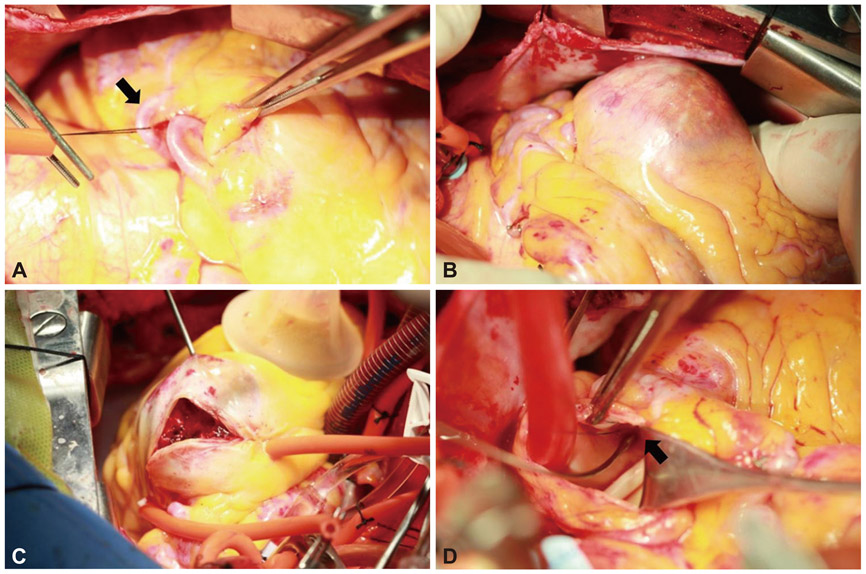
Fig. 5 Operative photograph. A: a fistula from the conus artery to pulmonary artery (arrow). B: aneurysmal sac. C: aneurysmal sac filled with thrombus. D: a fistula opening (arrow) at pulmonary artery.
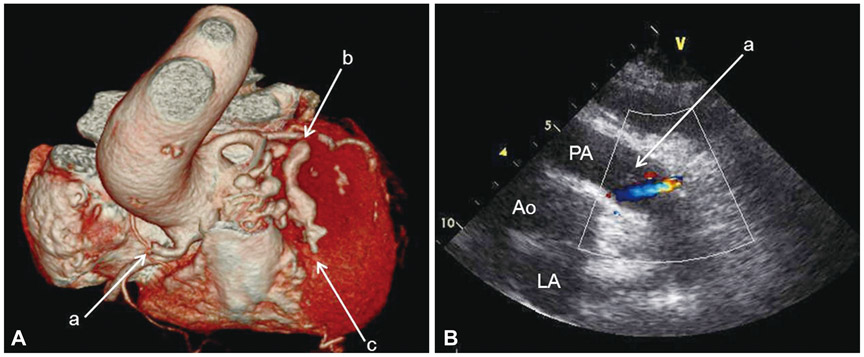
Fig. 6 Postoperative evaluation. A: coronary artery CT shows ligation sites. a: conus artery fistula ligation, b: LAD aneurysm proximal ligation, c: LAD aneurysm distal ligation. B: echocardiography shows remnant fistula. a: pulmonary valve. PA: pulmonary artery, Ao: aorta, LA: left atrium, LAD: left anterior descending artery.
Reference
-
1. Gziut AI, Gil RJ. Coronary aneurysms. Polskie Archiwum Medycyny Wewneętrznej. 2008. 118:741–745.2. Anné W, Bogaert J, Van de Werf F. A case report of a patient with a large aneurysmatic coronary artery fistula. Acta Cardiol. 2000. 55:307–310.3. Hirooka K, Hanatani A, Nakatani S, et al. Huge saccular aneurysm in a coronary-pulmonary fistula fed by the left and right coronary arteries. Circ J. 2002. 66:525–527.4. Ueno T, Nakayama Y, Yoshikai M, et al. Unique manifestations of congenital coronary artery fistulas. Am Heart J. 1992. 124:1388–1391.5. Syed M, Lesch M. Coronary artery aneurysm: a review. Prog Cardiovasc Dis. 1997. 40:77–84.6. Nichols L, Lagana S, Parwani A. Coronary artery aneurysm: a review and hypothesis regarding etiology. Arch Pathol Lab Med. 2008. 132:823–828.7. Markis JE, Joffe CD, Cohn PF, Feen DJ, Herman MV, Gorlin R. Clinical significance of coronary arterial ectasia. Am J Cardiol. 1976. 37:217–222.8. Daoud AS, Pankin D, Tulgan H, Florentin RA. Aneurysms of the coronary artery. Report of ten cases and review of literature. Am J Cardiol. 1963. 11:228–237.9. Yu W, Yusa L, Shou H, Wei P, Tao Q. Surgical treatment of giant coronary artery aneurysm. Asian Cardiovasc Thorac Ann. 2001. 9:215–217.10. Li D, Wu Q, Sun L, et al. Surgical treatment of giant coronary artery aneurysm. J Thorac Cardiovasc Surg. 2005. 130:817–821.11. Kimura S, Miyamoto K, Ueno Y. Cardiac tamponade due to spontaneous rupture of large coronary artery aneurysm. Asian Cardiovasc Thorac Ann. 2006. 14:422–424.12. Gunduz H, Akdemir R, Binak E, Tamer A, Uyan C. Spontaneous rupture of a coronary artery aneurysm: a case report and review of the literature. Jpn Heart J. 2004. 45:331–336.13. Carr JA, Al-Sadir J, Jeevanandam V. Anomalous coronary to pulmonary artery fistula and aneurysm in an 86-year-old female. J Card Surg. 2006. 21:188–190.14. Nakamura K, Shiratori K, Hashimoto K. Giant saccular aneurysm of coronary arteriovenous fistula to the main pulmonary artery: intraoperative assessment by using fluorescent imaging. Ann Thorac Cardiovasc Surg. 2010. 16:354–357.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Bilateral Coronary to Pulmonary Artery Fistulae with a Saccular Aneurysm: A case report
- Right Coronary Artery to Left Ventricular Fistula with a Giant Right Coronary Artery Aneurysm: A case report
- A Case of Coronary Artery Aneurysm
- Congenital coronary arteriovenous fistulae
- Coronary Artery Fistula with Giant Aneurysm and Coronary Stenosis Treated by Transcatheter Embolization and Stent
