Tako-Tsubo Cardiomyopathy by Transient Dynamic Left Midventricular Obstruction
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. dgpark@hallym.or.kr
- KMID: 1769512
- DOI: http://doi.org/10.4070/kcj.2009.39.1.37
Abstract
- A 48-year-old woman visited the emergency department with shock due to a urinary tract infection. The patient, who had a history of hypertension and diabetes mellitus, presented with precordial ST-segment elevation and Q waves, along with an increase of cardiac enzymes. An echocardiography showed moderately reduced systolic function, severe apical left ventricular ballooning, and a dynamic left ventricular outflow tract obstruction with a pressure gradient of 109 mmHg. Coronary angiography demonstrated normal coronary arteries. At the 1-month echocardiographic follow-up, the apical ballooning and left ventricular systolic function had recovered completely. There was no residual left ventricular intra-cavity gradient at rest, but it was induced in low-dose dobutamine stress-echocardiography. We demonstrated that dynamic left midventricular obstruction in the setting of either increased catecholamine stress or hypovolemia could develop Tako-tsubo cardiomyopathy.
MeSH Terms
Figure
-
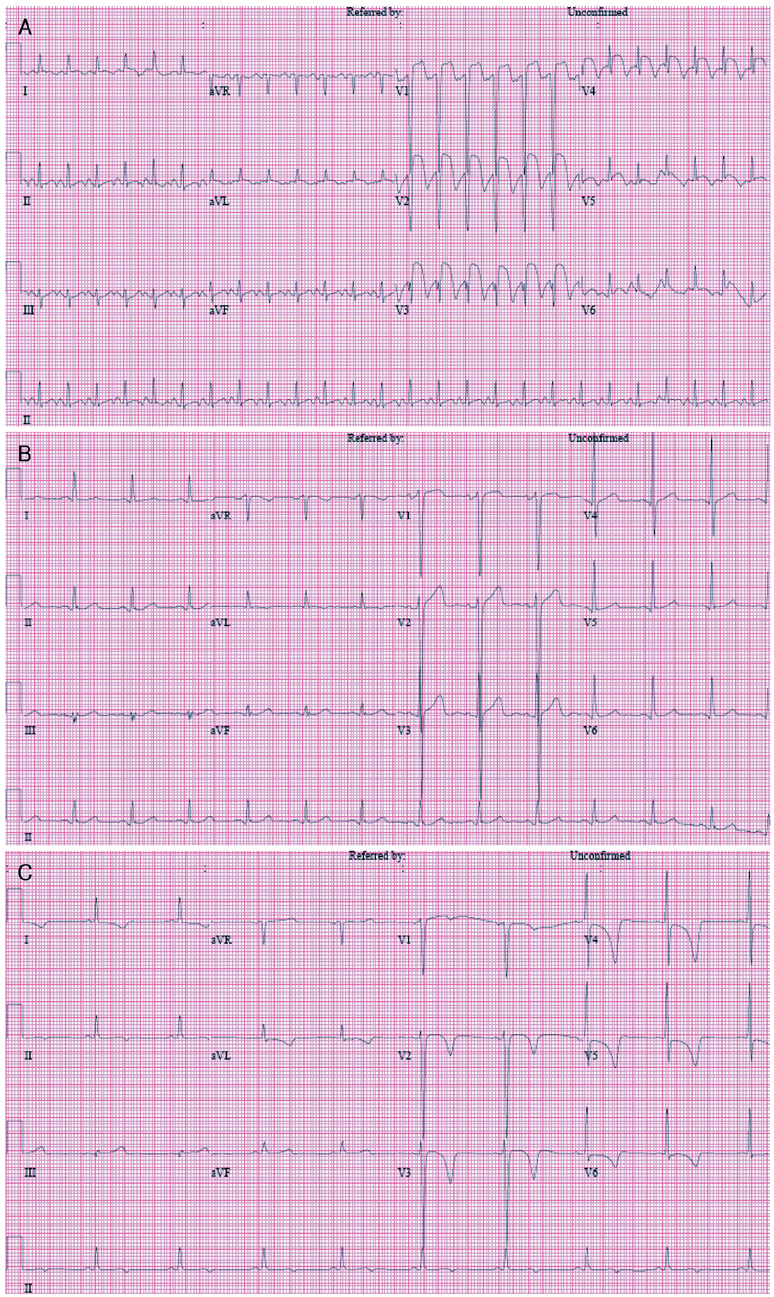
Fig. 1 Change of electrocardiographic finding over the course. A: electrocardiography on admission, showing ST-segment elevation with Q waves in V1-V4, I, and aVL. B: electrocardiography 3 months before admission, showing left ventricular hypertrophy. C: electrocardiography on day 28, showing T wave inversion in V2-6.
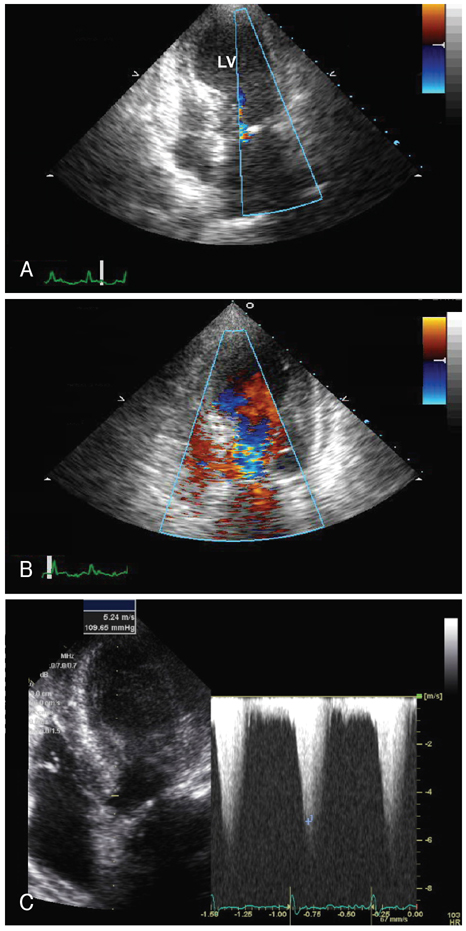
Fig. 2 Initial echocardiography on admission. A: end-systolic echocardiogram, showing left ventricular apical ballooning. B: end-diastolic echocardiogram, showing flow acceleration in the left ventricular outflow tract. C: continuous wave Doppler ultrasound showing a left ventricular outflow tract pressure gradient of 109 mmHg.
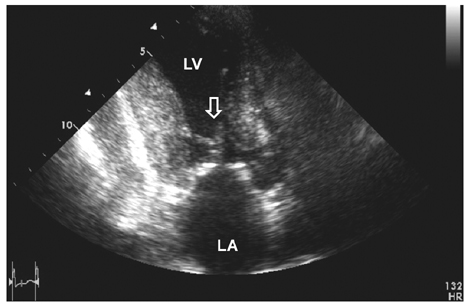
Fig. 3 Echocardiography on day 5, showing systolic anterior motion of the mitral valve (arrow).
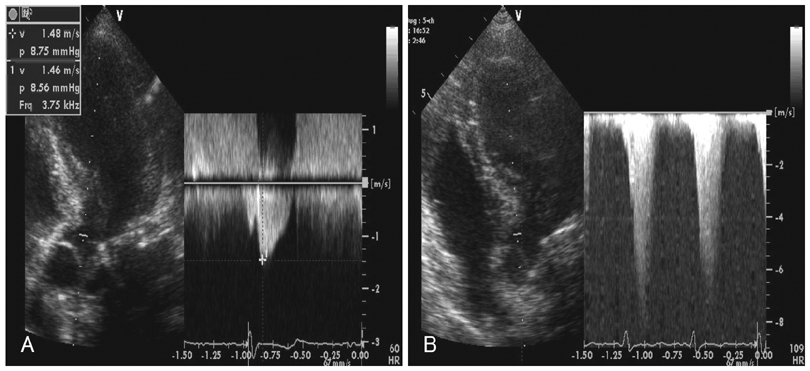
Fig. 4 Dobutamine stress echocardiography on day 28. A: baseline echocardiography. B: at the peak dose, a dynamic left ventricular mid-cavity obstruction with a pressure gradient of 158 mmHg was induced. This gradient resolved during the recovery period.
Cited by 1 articles
-
Different Characteristics between Patients with Apical and Non-Apical Subtypes of Stress-Induced Cardiomyopathy
Sun Hwa Lee, Won Ho Kim, Sang Rok Lee, Kyung Suk Rhee, Jei Keon Chae, Jae Ki Ko
J Cardiovasc Ultrasound. 2013;21(3):116-122. doi: 10.4250/jcu.2013.21.3.116.
Reference
-
1. Merli E, Sutcliffe S, Gori M, Sutherland GG. Tako-tsubo cardiomyopathy: new insights into the possible underlying pathophysiology. Eur J Echocardiogr. 2006. 7:53–61.2. Villareal RP, Achari A, Wilansky S, Wilson JM. Anteroapical stunning and left ventricular outflow tract obstruction. Mayo Clin Proc. 2001. 76:79–83.3. Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol. 2001. 38:11–18.4. Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005. 352:539–548.5. Cocco G, Chu D. Stress-induced cardiomyopathy: a review. Eur J Intern Med. 2007. 18:369–379.6. Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: first series in white patients. Heart. 2003. 89:1027–1031.7. Lee HH, Gwon HC, Kim BJ, et al. Clinical manifestation of novel stress-induced cardiomyopathy mimicking acute myocardial infarction: single center prospective registry. Korean Circ J. 2002. 32:1054–1063.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tako-Tsubo Cardiomyopathy Triggered by Misdirection
- A Case of Pheochromocytoma-induced Reverse Tako-Tsubo Cardiomyopathy: Insights from Multimodal Imaging
- Tako-tsubo Syndrome after Acute Traumatic Subdural Hematoma Mimicking Acute ST Elevation Myocardial Infarction
- 4 Cases of Midventricular Obstructive Hypertrophic Obstructive Cardiomyopathy
- A Unique Case of Transient Midventricular Ballooning: An Atypical Manifestation of Stress-Induced Cardiomyopathy Involving Both Ventricles
