The Role of PET/CT for Evaluating Breast Cancer
- Affiliations
-
- 1Department of Radiology, College of Medicine Seoul National University and The Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea. moonwk@radcom.snu.ac.kr
- KMID: 1734292
- DOI: http://doi.org/10.3348/kjr.2007.8.5.429
Abstract
- Positron emission tomography combined with computed tomography (PET/CT) has been receiving increasing attention during the recent years for making the diagnosis, for determining the staging and for the follow-up of various malignancies. The PET/CT findings of 58 breast cancer patients (age range: 34-79 years old, mean age: 50 years) were retrospectively compared with the PET or CT scans alone. PET/CT was found to be better than PET or CT alone for detecting small tumors or multiple metastases, for accurately localizing lymph node metastasis and for monitoring the response to chemotherapy in breast cancer patients.
MeSH Terms
-
Adult
Aged
Bone Neoplasms/*diagnosis/pathology/secondary
Breast/pathology/radionuclide imaging
Breast Neoplasms/*diagnosis/pathology/radionuclide imaging
Carcinoma, Ductal, Breast/diagnosis/pathology
Carcinoma, Intraductal, Noninfiltrating/*diagnosis/pathology/radionuclide imaging
Contrast Media/administration & dosage
Female
Humans
Lymphatic Metastasis
Mammography/methods
Middle Aged
Neoplasm Recurrence, Local/*diagnosis/pathology
Neoplasm Staging/methods
Positron-Emission Tomography/*methods
Radiographic Image Enhancement/methods
Reproducibility of Results
Retrospective Studies
Sensitivity and Specificity
Tomography, X-Ray Computed/*methods
Ultrasonography, Mammary
Figure
-
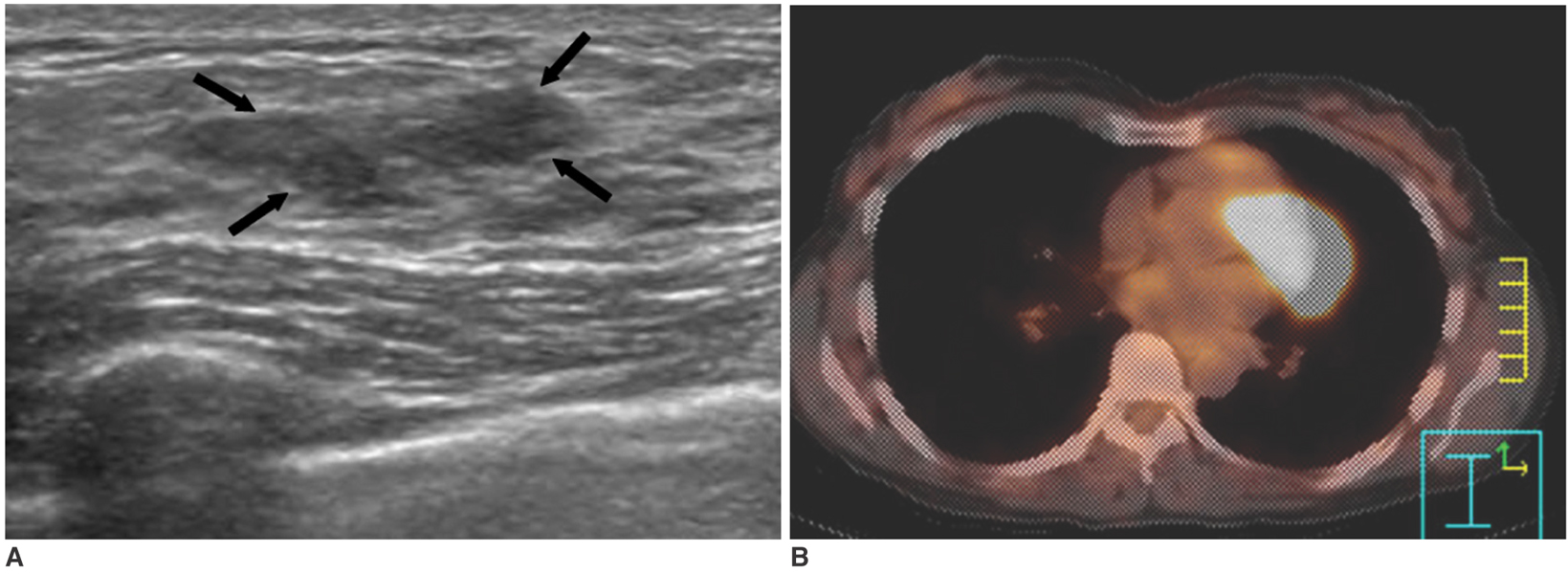
Fig. 1 Ductal carcinoma in situ in a 49-year-old woman. A. Sonography shows a 2.5 cm sized hypoechoic mass with an indistinct margin in the left upper breast (arrows). B. The PET/CT image shows no evidence of FDG uptake in the left breast. Surgery revealed ductal carcinoma in situ.
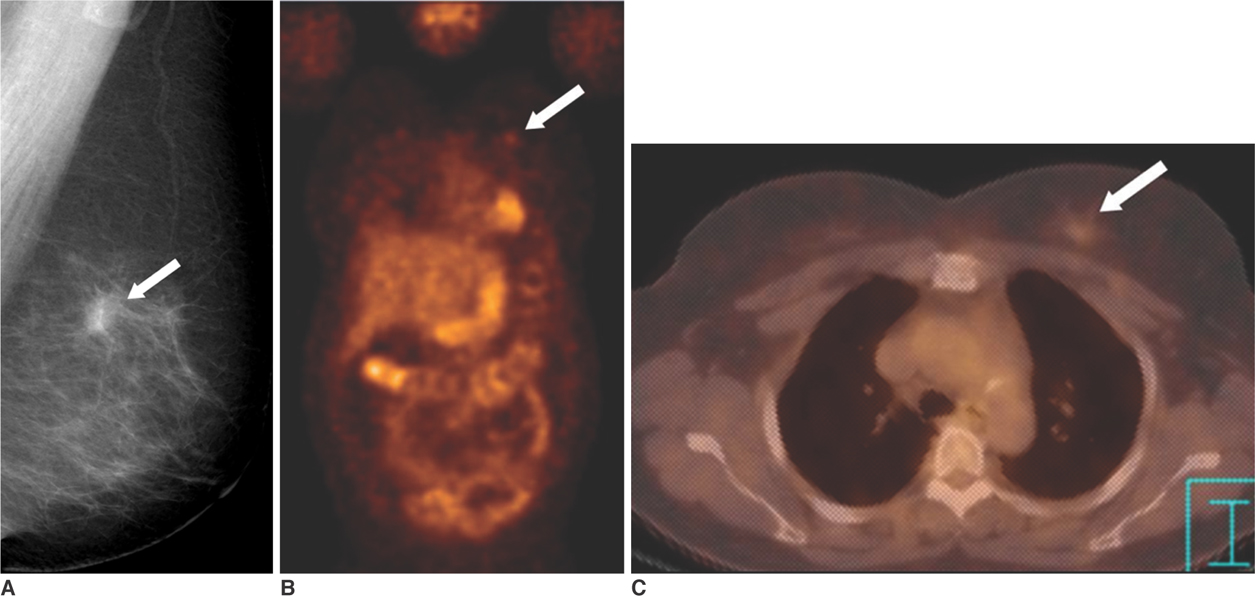
Fig. 2 Invasive breast cancer in a 57-year-old woman. A. The mediolateral oblique view of the screening mammogram shows a 1.1 cm sized spiculated mass (arrow) in the left breast. B. The PET image shows faint FDG uptake (SUV = 1.2) (arrow) in the left breast. It is difficult to detect the lesion due to partial volume averaging. C. The PET/CT image shows that the focal uptake (arrow) is localized to the left breast.
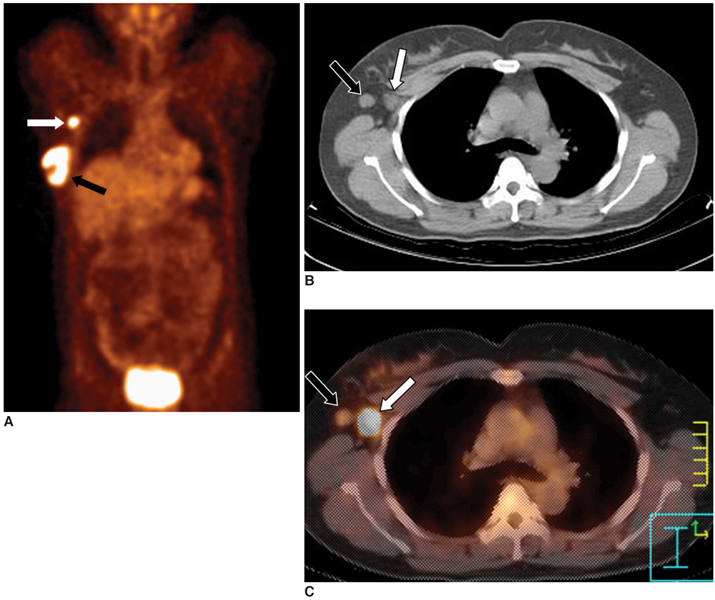
Fig. 3 Axillary lymph node metastasis in a 45-year-old woman with a 4 cm invasive ductal carcinoma. A. The PET image shows increased FDG uptake in the right breast (black arrow) and axilla (white arrow). B. The CT image shows two enlarged lymph nodes in the right axilla (arrows). C. The PET/CT image shows accurate localization of the metastatic (white arrow, SUV = 9.9) and reactive (black arrow) lymph nodes. Surgery revealed one metastatic lymph node out of the 21 excised axillary lymph nodes.
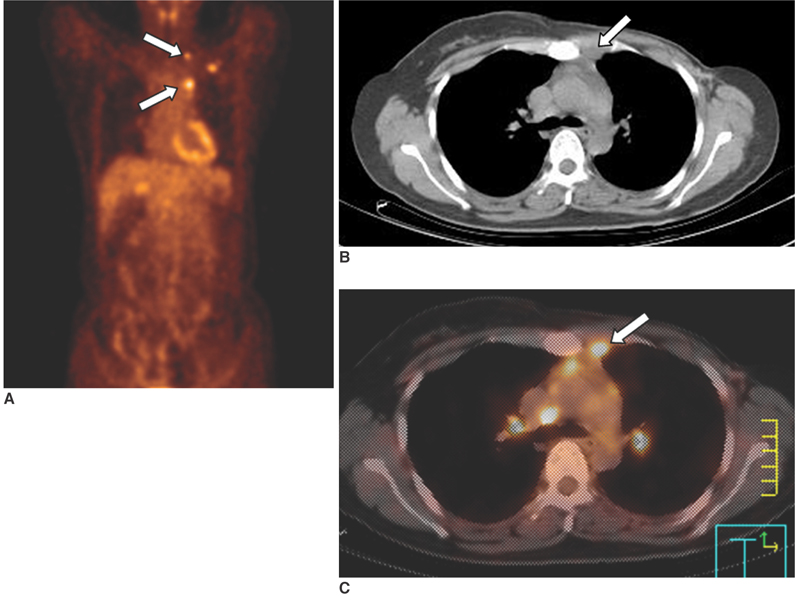
Fig. 4 Mediastinal lymph node metastasis in a 41-year-old woman who had undergone left modified radical mastectomy 10 months previously. A. The PET image shows multiple areas of increased uptake (arrows) in the left upper chest. B. The CT image shows a small soft tissue density in the anterior mediastinum (arrow). C. The PET/CT image shows co-registration of the FDG uptake and the soft tissue density in the anterior mediastinum, suggesting internal mammary lymph node metastases (arrow).
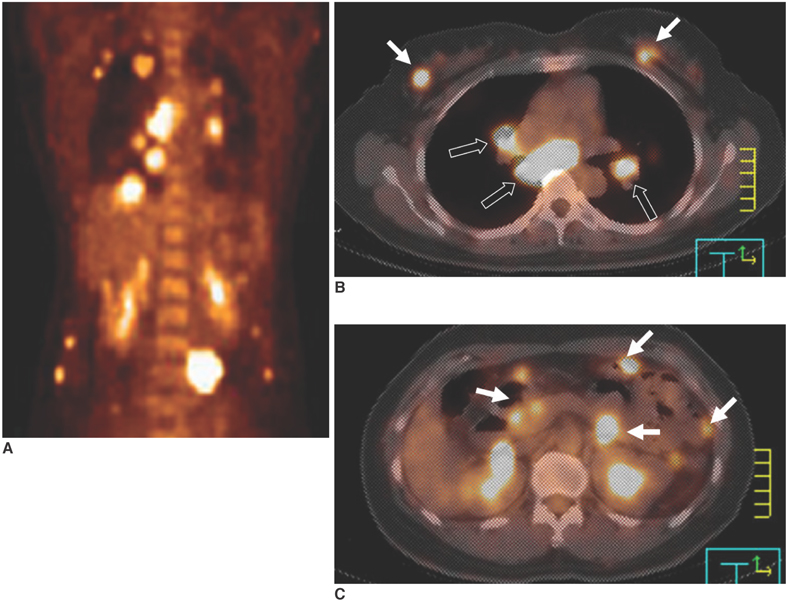
Fig. 5 Multiple distant metastases in a 44-year-old woman with bilateral breast cancer. A. The PET image shows multiple areas of FDG uptake in the thorax and abdomen. B, C. The PET/CT images show high uptake in both breasts (white arrows in B), the mediastinal lymph nodes (black arrows in B) and the visceral organs (arrows in C).

Fig. 6 Bone metastases in a 47-year-old woman with breast cancer. A-C. The PET and PET/CT images show increased FDG uptake in the T5 (B) and L1 (C) vertebrae (arrows). Osteolytic changes suggestive of bone metastases are seen on CT. D. The whole body Tc-99m bone scintigram obtained 7 days before the PET scan shows faint uptake in only the L1 vertebra (arrow). T5 metastasis is not visualized. E. The follow-up bone scintigram obtained three months later shows foci of hot uptake in the T5 and L1 vertebrae (arrows). PET/CT was superior to bone scintigram for the early detection of osteolytic breast cancer metastasis.
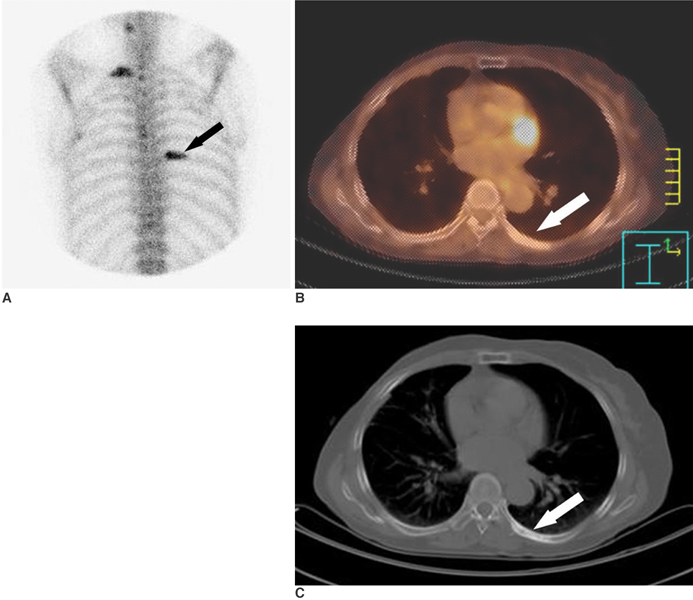
Fig. 7 Bone metastases in a 64-year-old woman who had undergone right modified radical mastectomy 36 months previously. A. The bone scintigram shows increased FDG uptake in the right 1st and left 7th ribs (arrow), which is probably due to bony metastases. B. The PET/CT image shows no FDG uptake in the left 7th rib (arrow). C. The CT image shows an osteoblastic bony lesion in the left 7th rib (arrow).
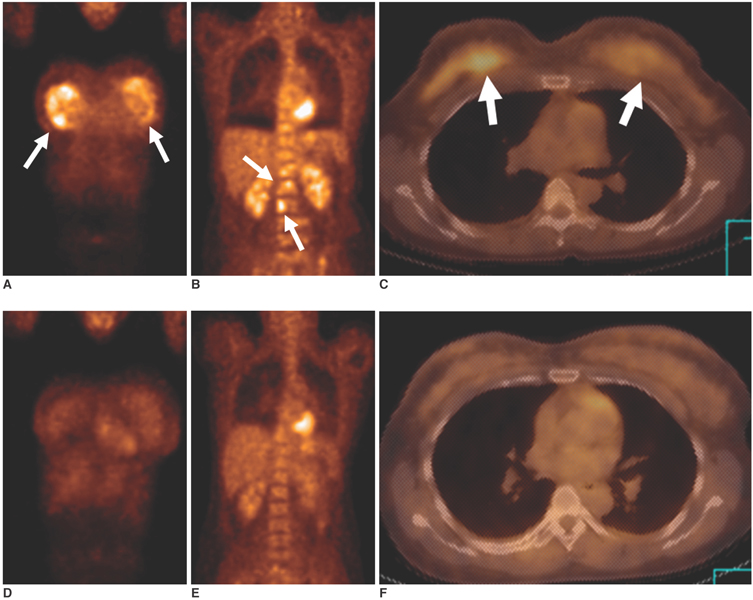
Fig. 8 Chemotherapy in a 35-year-old woman with bilateral breast cancer and bone metastases. A-C. The initial PET (A, B) and PET/CT (C) images show strong FDG uptake (arrows) in both breasts and in multiple spinal levels. D-F. The follow-up PET (D, E) and PET/CT (F) images obtained after three cycles of chemotherapy show markedly decreased FDG uptake in both breasts and in multiple spinal levels.
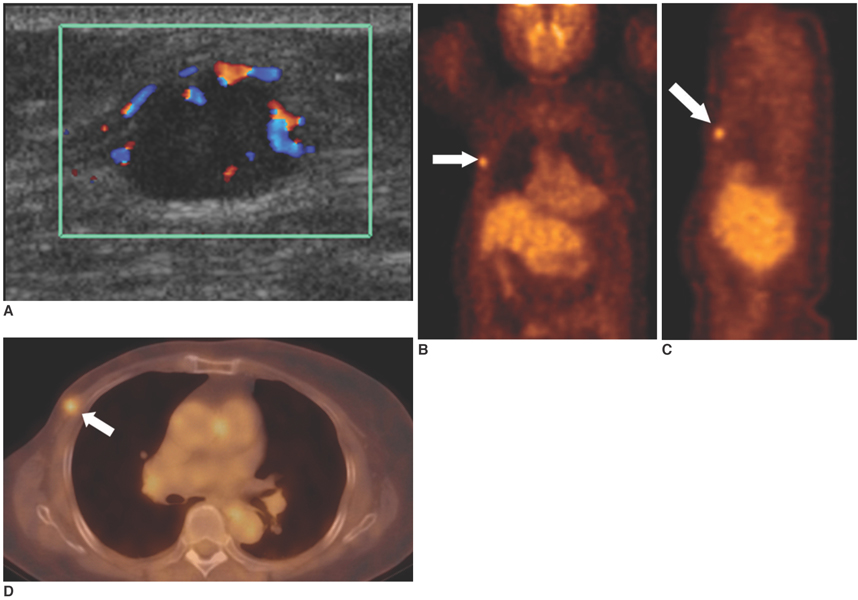
Fig. 9 Local recurrence in a 74-year-old woman who had undergone right modified radical mastectomy eight years previously. A. Sonography shows an 1.4 cm oval mass with increased vascularity in the right pectoralis muscle at the mastectomy site. B, C. The PET images show focal high FDG uptake (SUV= 3.3) (arrows) in the right chest wall. D. The PET/CT image shows a focus of high FDG uptake (arrow) localized to the right pectoralis muscle. Accurate localization of the lesion was difficult with using PET alone.
Reference
-
1. Minn H, Soini I. F-18 fluorodeoxyglucose scintigraphy in diagnosis and follow up of treatment in advanced breast cancer. Am J Clin Pathol. 1989. 91:535–541.2. Kubota K, Matsuzawa T, Amemiya A, Kondo M, Fujiwara T, Watanuki S, et al. Imaging of breast cancer with F-18 fluorodeoxyglucose and positron emission tomography. J Comput Assist Tomogr. 1989. 13:1097–1098.3. Wahl RL, Cody RL, Hutchins GD, Mudgett EE. Primary and metastatic breast carcinoma: initial clinical evaluation with PET with the radiolabeled glucose analogue 2-[F-18]-fluoro-2-deoxy-D-glucose. Radiology. 1991. 179:765–770.4. Kostakoglu L, Goldsmith SJ. 18F-FDG PET evaluation of the response to therapy for lymphoma and for breast, lung, and colorectal carcinoma. J Nucl Med. 2003. 44:224–239.5. Beyer T, Townsend DW, Brun T, Kinahan PE, Charron M, Roddy R, et al. A combined PET/CT scanner for clinical oncology. J Nucl Med. 2000. 41:1369–1379.6. Ell PJ, Von Schulthess GK. PET/CT: a new road map. Eur J Nucl Med Mol Imaging. 2002. 29:719–720.7. Tatsumi M, Cohade C, Mourtzikos KA, Fishman EK, Wahl RL. Initial experience with FDG-PET/CT in the evaluation of breast cancer. Eur J Nucl Med Mol Imaging. 2006. 33:254–262.8. Lind P, Igerc I, Beyer T, Reinprecht P, Hausegger K. Advantages and limitations of FDG PET in the follow-up of breast cancer. Eur J Nucl Med Mol Imaging. 2004. 31:Suppl1. S125–S134.9. Fueger BJ, Weber WA, Quon A, Crawford TL, Allen-Auerbach MS, Halpern BS, et al. Performance of 2-Deoxy-2-[F-18]fluoro-D-glucose positron emission tomography and integrated PET/CT in restaged breast cancer patients. Mol Imaging Biol. 2005. 7:369–376.10. Avril N, Rosé CA, Schelling M, Dose J, Kuhn W, Bense S, et al. Breast imaging with positron emission tomography and fluorine-18 fluorodeoxyglucose: use and limitations. J Clin Oncol. 2000. 18:3495–3502.11. Schirrmeister H, Kühn T, Guhlmann A, Santjohanser C, Hörster T, Nüssle K, et al. Fluorine-18 2-deoxy-2-fluoro-D-glucose PET in the preoperative staging of breast cancer: comparison with the standard staging procedures. Eur J Nucl Med. 2001. 28:351–358.12. Noh DY, Yun IJ, Kang HS, Kim YC, Kim JS, Chung JK, et al. Detection of cancer in augmented breast by positron emission tomography. Eur J Surg. 1999. 165:847–851.13. Bar-Shalom R, Yefremov N, Guralnik L, Gaitini D, Frenkel A, Kuten A, et al. Clinical performance of PET/CT in evaluation of cancer: additional value for diagnostic imaging and patient management. J Nucl Med. 2003. 44:1200–1209.14. Greco M, Crippa F, Agresti R, Seregni E, Gerali A, Giovanazzi R, et al. Axillary lymph node staging in breast cancer by 2-fluoro-2-deoxy-D-glucose positron emission tomography: clinical evaluation and alternative management. J Natl Cancer Inst. 2001. 93:630–635.15. Eubank WB, Mankoff DA, Takasugi J, Vesselle H, Eary JF, Shanley TJ, et al. 18fluorodeoxyglucose positron emission tomography to detect mediastinal or internal mammary metastases in breast cancer. J Clin Oncol. 2001. 19:3516–3523.16. Moon DH, Maddahi J, Silverman DH, Glaspy JA, Phelps ME, Hoh CK. Accuracy of whole-body fluorine-18-FDG PET for the detection of recurrent or metastatic breast carcinoma. J Nucl Med. 1998. 39:431–435.17. Cook GJ, Houston S, Rubens R, Maisey MN, Fogelman I. Detection of bone metastases in breast cancer by 18FDG PET: differing metabolic activity in osteoblastic and osteolytic lesions. J Clin Oncol. 1998. 16:3375–3379.18. Uematsu T, Yuen S, Yukisawa S, Aramaki T, Morimoto N, Endo M, et al. Comparison of FDG PET and SPECT for detection of bone metastases in breast cancer. AJR Am J Roentgenol. 2005. 184:1266–1273.19. Heys SD, Eremin JM, Sarkar TK, Hutcheon AW, Ah-See A, Eremin O. Role of multimodality therapy in the management of locally advanced carcinoma of the breast. J Am Coll Surg. 1994. 179:493–504.20. Smith IC, Welch AE, Hutcheon AW, Miller ID, Payne S, Chilcott F, et al. Positron emission tomography using [18F]-fluorodeoxy-D-glucose to predict the pathologic response of breast cancer to primary chemotherapy. J Clin Oncol. 2000. 18:1676–1688.21. Rése C, Dose J, Avril N. Positron emission tomography for the diagnosis of breast cancer. Nucl Med Commun. 2002. 23:613–618.22. Bradley J, Thorstad WL, Mutic S, Miller TR, Dehdashti F, Siegel BA, et al. Impact of FDG-PET on radiation therapy volume delineation in non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004. 59:78–86.23. Eubank WB, Mankoff DA, Vesselle HJ, Eary JF, Schubert EK, Dunnwald LK, et al. Detection of locoregional and distant recurrences in breast cancer patients by using FDG PET. RadioGraphics. 2002. 22:5–17.24. Kamby C, Vejborg I, Kristensen B, Olsen LO, Mouridsen HT. Metastatic pattern in recurrent breast cancer. special reference to intrathoracic recurrences. Cancer. 1988. 62:2226–2233.25. Grahek D, Montravers F, Kerrou K, Aide N, Lotz JP, Talbot JN. [18 F]FDG in recurrent breast cancer: diagnostic performances, clinical impact and relevance of induced changes in management. Eur J Nucl Med Mol Imaging. 2004. 31:179–188.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypermetabolic Axillary Mass on 18F FDG PET/CT: Breast Cancer Arising from Accessory Breast Tissue
- The Role of fluorodeoxyglucose PET in the management of breast cancer
- Use of 18F-FDG PET/CT in Second Primary Cancer
- Role of ¹â¸F-FDG PET-CT in Monitoring the Cyclophosphamide Induced Pulmonary Toxicity in Patients with Breast Cancer: 2 Case Reports
- Unusual Contralateral Axillary Lymph Node Metastasis in a Second Primary Breast Cancer Detected by FDG PET/CT and Lymphoscintigraphy
