J Korean Med Sci.
2004 Oct;19(5):753-755. 10.3346/jkms.2004.19.5.753.
A Case of Lambert-Eaton Myasthenic Syndrome Associated with Atypical Bronchopulmonary Carcinoid Tumor
- Affiliations
-
- 1Department of Neurology, College of Medicine, Pusan National University, Busan, Korea. dskim@pusan.ac.kr
- 2Department of Pulmonology, College of Medicine, Pusan National University, Busan, Korea.
- 3Department of Pathology, College of Medicine, Pusan National University, Busan, Korea.
- KMID: 1733522
- DOI: http://doi.org/10.3346/jkms.2004.19.5.753
Abstract
- The Lambert-Eaton myasthenic syndrome (LEMS) is typically recognized as a paraneoplastic syndrome associated with a small cell lung carcinoma (SCLC), whereas LEMS with other neuroendocrine lung tumors, including carcinoids or large cell lung carcinoma, are highly unusual. Here, we report a rare case of LEMS with atypical bronchopulmonary carcinoid tumor: A 65-yr-old man presented with progressive leg weakness and a diagnosis of LEMS was made by serial repetitive nerve stimulation test. Chest CT revealed a lung nodule with enlargement of paratracheal lymph nodes, and surgically resected lesion showed pathological features of atypical carcinoid tumor. We concluded that LEMS could be associated with rare pulmonary neuroendocrine tumor other than SCLC, which necessitates pathologic confirmation followed by aggressive treatment for optimal management in these rare cases.
MeSH Terms
Figure
-

Fig. 1 Postexercise fascilitation and incremental response at high rate of stimuration in the abductor digiti minimi muscle. Note definite facilitation at high rate of stimulation is achieved by prolonged stimulation for 2 sec in second test. (A) Compound muscle action potential (CMAP) before exercise. (B) CMAP after 30 sec of exercise. (C) Response at 50/sec stimulation for 1 sec. (D) Response at 50/sec stimulation for 2 sec.
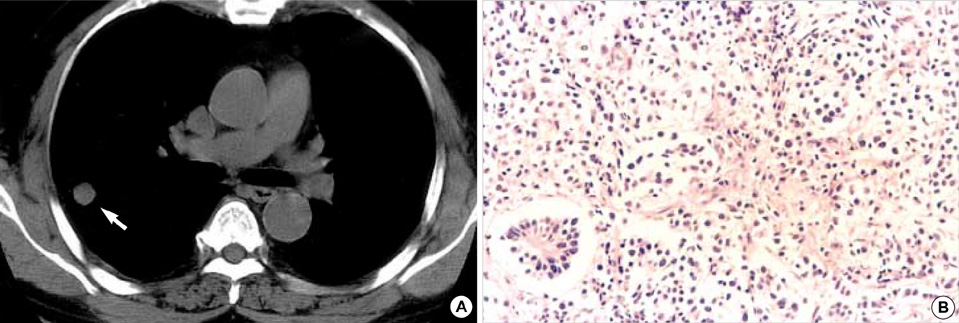
Fig. 2 (A) CT scan of the chest shows a 1.4 cm nodule (arrow) in the posterior segment of right upper lobe. (B) Atypical carcinoid tumor with mosaic patterns separated by thin fibrovascular stroma. The tumor cells have central round nuclei with abundant cytoplasm (H&E ×100).
Reference
-
1. Burns TM, Juel VC, Sanders DB, Phillips LH II. Neuroendocrine lung tumors and disorders of the neuromusclular junction. Neurology. 1999. 52:1490–1491.2. Elrington G, Newsom-Davis J. Lisak RP, editor. Clinical presentation and current immunology of the Lambert-Eaton myasthenic syndrome. Handbook of Myasthenia Gravis and Myasthenic Syndromes. 1994. New York: Marcel Dekker;81–102.3. Gutmann L, Phillips LH 2nd, Gutmann L. Trends in the association of Lambert-Eaton myasthenic syndrome with carcinoma. Neurology. 1992. 42:848–850.
Article4. Oh SJ. Principles of Clinical Electromyography, Case studies. 1998. Baltimore, USA: Williams & Wilkins.5. Tim RW, Massey JM, Sanders DB. Lambert-Eaton myasthenic syndrome: Electrodiagnostic findings and response to treatment. Neurology. 2000. 54:2176–2178.
Article6. Corrin B. Pathology of the Lungs. 2000. London: Churchil-Livingstone.7. Sanders DB. Lambert-Eaton myasthenic syndrome: clinical diagnosis, immune-mediated mechanisms, and update on therapies. Ann Neurol. 1995. 37:Suppl 1. S63–S73.
Article8. Oh SJ. Diverse electrophysiological spectrum of the Lambert-Eaton myasthenic syndrome. Muscle & Nerve. 1989. 12:464–469.
Article9. Moon JS, Sunwoo IN, Kim SM, Lee SA, Cho KH, Park KD, Kim WK, Choi BO, Chun HY. Clinical analysis of 12 Korean Lambert-Eaton myasthenic syndrome (LEMS) patients. Yonsei Med J. 1999. 40:454–459.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Marked Improvement of Lambert-Eaton Myasthenic Syndrome with the Chemotherapy of Small Cell Lung Carcinoma
- Electrophysiological Changes in Lambert-Eaton Myasthenic Syndrome With Intravenous Immunoglobulin Therapy
- A Diagnostic Dilemma: Normal Repetitive Nerve Stimulation in Lambert-Eaton Myasthenic Syndrome
- Lambert-Eaton Myasthenic Syndrome (LEMS) Presented With Ocular Symptoms
- Lambert-Eaton Myasthenic Syndrome Presenting as Cerebellar Symptoms
