Percutaneous Radiologic Gastrostomy Using the One-Anchor Technique in Patients after Partial Gastrectomy
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 138-736, Korea. jhshin@amc.seoul.kr
- KMID: 1731053
- DOI: http://doi.org/10.3348/kjr.2014.15.4.488
Abstract
OBJECTIVE
The purpose of our study was to assess the feasibility of performing percutaneous radiologic gastrostomy (PRG) in patients who had undergone partial gastrectomy and to evaluate factors associated with technical success.
MATERIALS AND METHODS
Nineteen patients after partial gastrectomy, who were referred for PRG between April 2006 and April 2012, were retrospectively analyzed. The remnant stomach was punctured using a 21-gauge Chiba-needle. A single anchor was used for the gastropexy and a 12-Fr or 14-Fr gastrostomy tube was inserted. Data were collected regarding the technical success, procedure time, and presence of any complications. Univariable analyses were performed to determine the factors related to the technical success.
RESULTS
Percutaneous radiologic gastrostomy was technically successful in 10 patients (53%), while a failed attempt and failure without an attempt were observed in 5 (26%) and 4 (21%) patients, respectively. Percutaneous radiologic jejunostomy was successfully performed in 9 patients who experienced technical failure. In the 10 successful PRG cases, the mean procedure time was 6.35 minutes. Major complications occurred in 2 patients, tube passage through the liver and pneumoperitonum in one and severe hemorrhage in the other. The technical success rate was higher in patients with Billroth I gastrectomy (100%, 6/6) than in patients with Billroth II gastrectomy (31%, 4/13) (p = 0.011).
CONCLUSION
Percutaneous radiologic gastrostomy can be successfully performed using the one-anchor technique in approximately half of the patients after partial gastrectomy.
Keyword
MeSH Terms
Figure
-
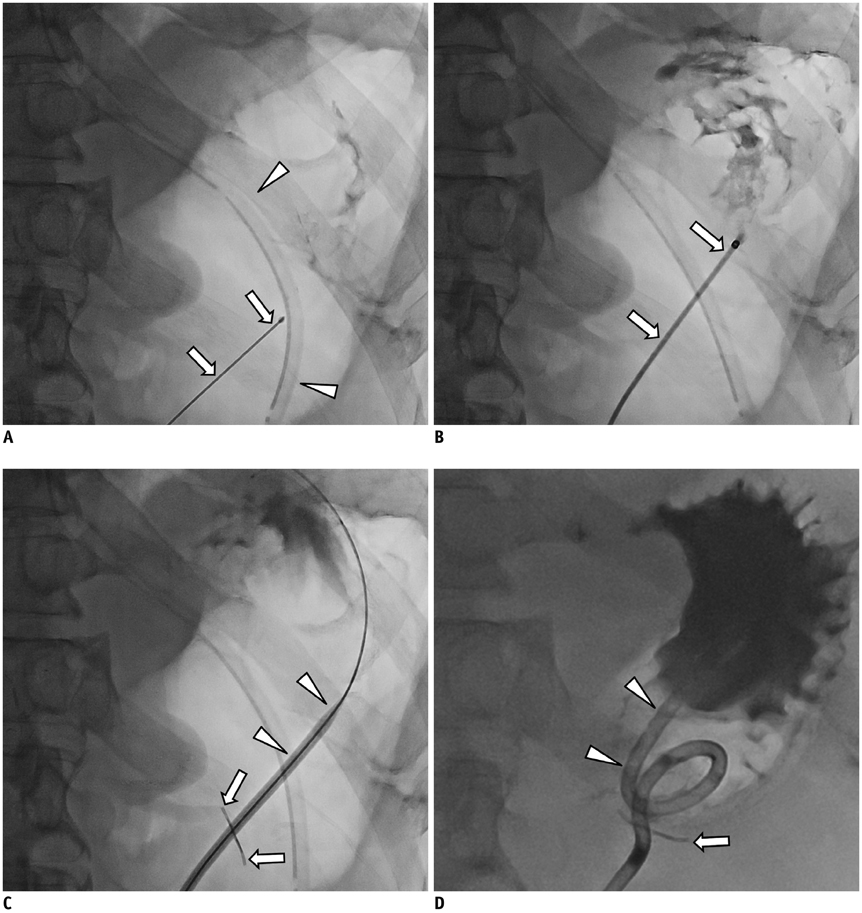
Fig. 1 Successful percutaneous radiologic gastrostomy in patient with distal gastrectomy with gastroduodenostomy. A. Chiba needle (arrows) is advanced into remnant stomach which was inflated with 250 mL of air through nasogastric tube (arrowheads). Intragastric location of Chiba needle is confirmed with contrast injection. B. Chiba needle is then exchanged for Neff catheter (arrows) using 0.018-inch guide wire. C. Cope suture anchor (arrows in C, D) is deployed into stomach through Neff catheter using 0.035-inch guide wire. Then puncture site is serially dilated using dilator (arrowheads). D. 14-Fr locking-loop catheter (arrowheads) is inserted into remnant stomach. There is good passage of contrast medium without leakage.
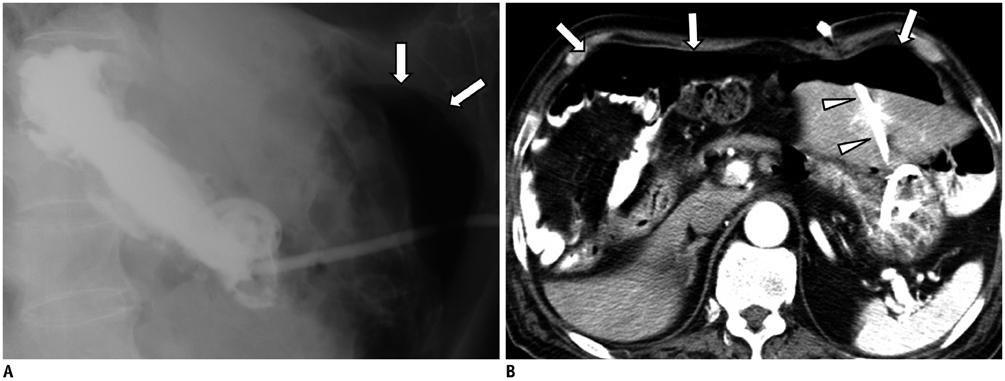
Fig. 2 Pneumoperitoneum developed three days following percutaneous radiologic gastrostomy (PRG). A. Lateral view, which was obtained three days after PRG, shows pneumoperitoneum (arrows). There was neither pneumoperitoneum nor contrast leakage on one-day follow-up radiograph (not shown). B. CT scan obtained three days after PRG shows large amount of pneumoperitoneum (arrows) as well as passage of gastrostomy tube through left hepatic lobe (arrowheads). Gastrostomy tube was removed with gradual resolution of pneumoperitoneum (not shown).
Reference
-
1. Deutsch LS, Kannegieter L, Vanson DT, Miller DP, Brandon JC. Simplified percutaneous gastrostomy. Radiology. 1992; 184:181–183.2. Ho SG, Marchinkow LO, Legiehn GM, Munk PL, Lee MJ. Radiological percutaneous gastrostomy. Clin Radiol. 2001; 56:902–910.3. Coleman CC, Coons HG, Cope C, Derauf BJ, Krenzel C, Epstein DH, et al. Percutaneous enterostomy with the Cope suture anchor. Radiology. 1990; 174(3 Pt 1):889–891.4. Given MF, Hanson JJ, Lee MJ. Interventional radiology techniques for provision of enteral feeding. Cardiovasc Intervent Radiol. 2005; 28:692–703.5. Silas AM, Pearce LF, Lestina LS, Grove MR, Tosteson A, Manganiello WD, et al. Percutaneous radiologic gastrostomy versus percutaneous endoscopic gastrostomy: a comparison of indications, complications and outcomes in 370 patients. Eur J Radiol. 2005; 56:84–90.6. Dewald CL, Hiette PO, Sewall LE, Fredenberg PG, Palestrant AM. Percutaneous gastrostomy and gastrojejunostomy with gastropexy: experience in 701 procedures. Radiology. 1999; 211:651–656.7. Given MF, Lyon SM, Lee MJ. The role of the interventional radiologist in enteral alimentation. Eur Radiol. 2004; 14:38–47.8. Lorentzen T, Nolsøe CP, Adamsen S. Percutaneous radiologic gastrostomy with a simplified gastropexy technique under ultrasonographic and fluoroscopic guidance: experience in 154 patients. Acta Radiol. 2007; 48:13–19.9. Shin JH, Song HY, Kim TH, Kim KR, Choi KE, Kim JH. Percutaneous radiologic gastrostomy: a modified Chiba-needle puncture technique with single gastropexy. Abdom Imaging. 2010; 35:189–194.10. Swetech J, Hasan S. Combined endoscopic and surgical modalities for percutaneous endoscopic gastrostomy placement in the setting of subtotal gastrectomy with a gastric pull up. Gastrointest Endosc. 1990; 36:316–317.11. Kurchin A, Halloran W, Kornfield R. Assessing the feasibility of percutaneous endoscopic gastrostomy following gastrectomy. Gastrointest Endosc. 1988; 34:366–367.12. Varney RA, vanSonnenberg E, Casola G, Sukthankar R. Balloon techniques for percutaneous gastrostomy in a patient with partial gastrectomy. Radiology. 1988; 167:69–70.13. Stellato TA, Gauderer MW, Ponsky JL. Percutaneous endoscopic gastrostomy following previous abdominal surgery. Ann Surg. 1984; 200:46–50.14. Singh P, Kahn D, Greenberg R, Indaram A, Pooran N, Bank S. Feasibility and safety of percutaneous endoscopic gastrostomy in patients with subtotal gastrectomy. Endoscopy. 2003; 35:311–314.15. Rosenzweig TB, Palestrant AM, Esplin CA, Gilsdorf RB. A method for radiologic-assisted gastrostomy when percutaneous endoscopic gastrostomy is contraindicated. Am J Surg. 1994; 168:587–590.16. Perona F, Castellazzi G, De Iuliis A, Rizzo L. Percutaneous radiologic gastrostomy: a 12-year series. Gut Liver. 2010; 4:Suppl 1. S44–S49.17. Yang ZQ, Shin JH, Song HY, Kwon JH, Kim JW, Kim KR, et al. Fluoroscopically guided percutaneous jejunostomy: outcomes in 25 consecutive patients. Clin Radiol. 2007; 62:1061–1065.18. Hu HT, Shin JH, Song HY, Kim JH, Yoon HK, Gwon DI, et al. Fluoroscopically guided percutaneous jejunostomy with use of a 21-gauge needle: a prospective study in 51 patients. J Vasc Interv Radiol. 2009; 20:1583–1587.19. Thornton FJ, Fotheringham T, Alexander M, Hardiman O, McGrath FP, Lee MJ. Amyotrophic lateral sclerosis: enteral nutrition provision--endoscopic or radiologic gastrostomy? Radiology. 2002; 224:713–717.20. Cantwell CP, Gervais DA, Hahn PF, Mueller PR. Feasibility and safety of infracolic fluoroscopically guided percutaneous radiologic gastrostomy. J Vasc Interv Radiol. 2008; 19:129–132.21. van Overhagen H, Ludviksson MA, Laméris JS, Zwamborn AW, Tilanus HW, Dees J, et al. US and fluoroscopic-guided percutaneous jejunostomy: experience in 49 patients. J Vasc Interv Radiol. 2000; 11:101–106.22. Seo N, Shin JH, Ko GY, Yoon HK, Gwon DI, Kim JH, et al. Incidence and management of bleeding complications following percutaneous radiologic gastrostomy. Korean J Radiol. 2012; 13:174–181.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Updates on Percutaneous Radiologic Gastrostomy/Gastrojejunostomy and Jejunostomy
- Percutaneous Radiologic Gastrostomy in a Locked-in Syndrome Patient : A case report
- Technique, Management and Complications of Percutaneous Endoscopic Gastrostomy
- Percutaneous Gastrostomy Tube Reinsertion after Accidental Dislodgement Using Modified Seldinger's Technique
- Recent update of percutaneous radiologic jejunostomy
