A Comparison of Arthroscopically Assisted Single and Double Bundle Tibial Inlay Reconstruction for Isolated Posterior Cruciate Ligament Injury
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yeungnam University College of Medicine, Daegu, Korea. ossoj@med.yu.ac.kr
- 2Department of Orthopaedic Surgery, Himchan Hospital, Seoul, Korea.
- KMID: 1719333
- DOI: http://doi.org/10.4055/cios.2010.2.2.76
Abstract
- BACKGROUND
This study evaluated the clinical results of arthroscopically assisted single and double bundle tibial inlay reconstructions of an isolated posterior cruciate ligament (PCL) injury.
METHODS
This study reviewed the data for 14 patients who underwent a single bundle tibial inlay PCL reconstruction (Group A) and 16 patients who underwent a double bundle tibial inlay PCL reconstruction (Group B) between August 1999 and August 2002. The mean follow-up period in groups A and B was 90.5 months and 64 months, respectively.
RESULTS
The Lysholm knee scores in groups A and B increased from an average of 43.3 +/- 7.04 and 44.7 +/- 5.02 preoperatively to 88.1 +/- 7.32 and 88.7 +/- 9.11 points at the final follow-up, respectively. In group A, stress radiography using a Telos device showed that the preoperative mean side-to-side differences (SSDs) of 9.5 +/- 1.60 mm at 30degrees of flexion and 9.8 +/- 1.70 mm at 90degrees of flexion were improved to 2.8 +/- 1.19 mm and 3.0 +/- 1.1 mm, respectively. In group B, the preoperative SSDs of 10.4 +/- 1.50 mm at 30degrees of flexion and 10.7 +/- 1.60 mm at 90degrees of flexion improved to 2.7 +/- 1.15 mm and 2.6 +/- 0.49 mm, respectively. There was no significant difference in the clinical scores and radiologic findings between the two groups.
CONCLUSIONS
Single bundle and double bundle PCL reconstructions using the tibial inlay technique give satisfactory clinical results in patients with an isolated PCL injury, and there are no significant differences in the clinical and radiological results between the two techniques. These results suggest that it is unnecessary to perform the more technically challenging double bundle reconstruction using the tibial inlay technique in an isolated PCL injury.
MeSH Terms
Figure
-
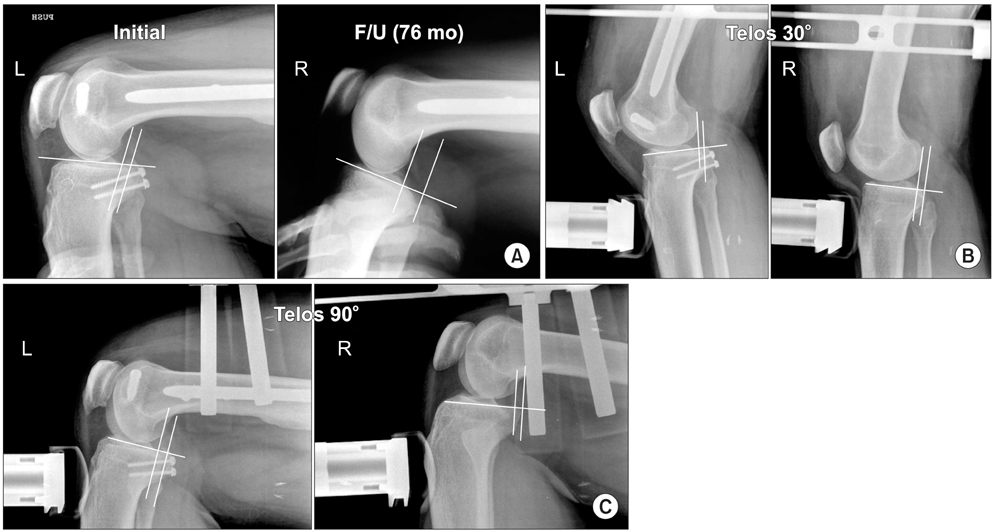
Fig. 1 Thirty-two year old man who was involved in a motor vehicle accident. Single bundle posterior cruciate ligament reconstruction was performed using the tibial inlay technique. (A) Stress view, preoperative and follow-up (F/U) 76 months. (B) Posterior stress roentgenography using the Telos stress device at 30° of flexion showed grade 1 posterior instability at both the preoperative and follow-up 76 months. (C) Posterior stress roentgenography using the Telos stress device at 90° of flexion showed grade 1 posterior instability at both the preoperative and follow-up 76 months.

Fig. 2 Forty-six year old man who was involved in a motor vehicle accident. A double bundle posterior cruciate ligament reconstruction was performed using the tibial inlay technique. (A) Stress view, preoperative and follow-up 60 months. (B) Posterior stress roentgenography using the Telos stress device at 30° of flexion showed grade 1 posterior instability both preoperatively and at the 60 months follow-up. (C) Posterior stress roentgenography using the Telos stress device at 90° of flexion showed grade 1 posterior instability preoperatively and at the 60 months follow-up.
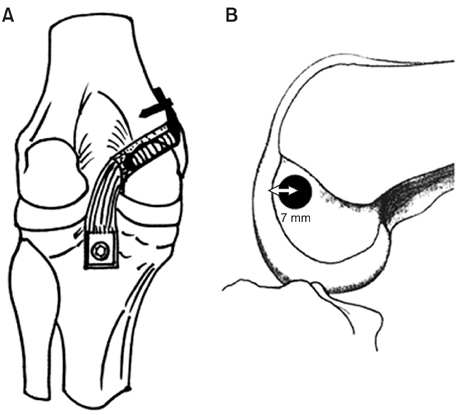
Fig. 3 (A) The illustration shows posterior view of a single bundle tibial inlay posterior cruciate ligament reconstruction. (B) Lateral view of femoral tunnel position in the medial femoral condyle. The center of a 10 mm diameter femoral tunnel was placed 7 mm proximal to the margin of the articular cartilage of the medial femoral condyle at 11 o'clock in the left knee joint, or at 1 o'clock in the right knee joint.
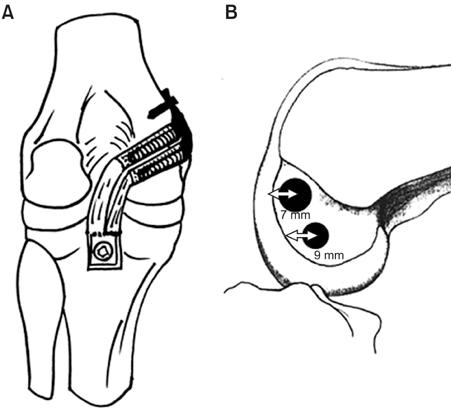
Fig. 4 (A) The illustration shows the posterior view of double bundle tibial inlay posterior cruciate ligament reconstructions. (B) Lateral view of the femoral tunnel position in the medial femoral condyle. The center for the 9 mm diameter anterolateral femoral tunnel was placed 7 mm proximal to the margin of the articular cartilage of the medial femoral condyle at the 11 o'clock position in the left knee joint, or at the 1 o'clock position in the right knee joint, and the center for 8 mm diameter posteromedial femoral tunnel, at 9 mm proximal to the margin of the articular cartilage at the 3 o'clock position on the right (9 o'clock on left). The distance between femoral tunnels must be > 4 mm to avoid tunnel bridge collapse.
Reference
-
1. Fanelli GC, Edson CJ. Posterior cruciate ligament injuries in trauma patients: part II. Arthroscopy. 1995. 11(5):526–529.
Article2. Shelbourne KD, Davis TJ, Patel DV. The natural history of acute, isolated, nonoperatively treated posterior cruciate ligament injuries: a prospective study. Am J Sports Med. 1999. 27(3):276–283.
Article3. Boynton MD, Tietjens BR. Long-term followup of the untreated isolated posterior cruciate ligament-deficient knee. Am J Sports Med. 1996. 24(3):306–310.
Article4. Clancy WG Jr, Shelbourne KD, Zoellner GB, Keene JS, Reider B, Rosenberg TD. Treatment of knee joint instability secondary to rupture of the posterior cruciate ligament: report of a new procedure. J Bone Joint Surg Am. 1983. 65(3):310–322.
Article5. Keller PM, Shelbourne KD, McCarroll JR, Rettig AC. Non-operatively treated isolated posterior cruciate ligament injuries. Am J Sports Med. 1993. 21(1):132–136.
Article6. MacGillivray JD, Stein BE, Park M, Allen AA, Wickiewicz TL, Warren RF. Comparison of tibial inlay versus transtibial techniques for isolated posterior cruciate ligament reconstruction: minimum 2-year follow-up. Arthroscopy. 2006. 22(3):320–328.
Article7. Seon JK, Song EK. Reconstruction of isolated posterior cruciate ligament injuries: a clinical comparison of the transtibial and tibial inlay techniques. Arthroscopy. 2006. 22(1):27–32.
Article8. Berg EE. Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy. 1995. 11(1):69–76.
Article9. Bergfeld JA, McAllister DR, Parker RD, Valdevit AD, Kambic HE. A biomechanical comparison of posterior cruciate ligament reconstruction techniques. Am J Sports Med. 2001. 29(2):129–136.
Article10. Markolf KL, Zemanovic JR, McAllister DR. Cyclic loading of posterior cruciate ligament replacements fixed with tibial tunnel and tibial inlay methods. J Bone Joint Surg Am. 2002. 84(4):518–524.
Article11. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000. 28(2):144–151.
Article12. Race A, Amis AA. The mechanical properties of the two bundles of the human posterior cruciate ligament. J Biomech. 1994. 27(1):13–24.
Article13. Shearn JT, Grood ES, Noyes FR, Levy MS. Two-bundle posterior cruciate ligament reconstruction: how bundle tension depends on femoral placement. J Bone Joint Surg Am. 2004. 86(6):1262–1270.
Article14. Fanelli GC, Giannotti BF, Edson CJ. The posterior cruciate ligament arthroscopic evaluation and treatment. Arthroscopy. 1994. 10(6):673–688.
Article15. Johnson DH, Fanelli GC, Miller MD. PCL 2002: indications, double-bundle versus inlay technique and revision surgery. Arthroscopy. 2002. 18:9 Suppl 2. 40–52.
Article16. Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res. 1985. (198):43–49.
Article17. L'Insalata JC, Harner CD. Treatment of acute and chronic posterior cruciate ligament deficiency: new approaches. Am J Knee Surg. 1996. 9(4):185–193.18. Miller MD, Olszewski AD. Posterior cruciate ligament injuries: new treatment options. Am J Knee Surg. 1995. 8(4):145–154.19. Sekiya JK, West RV, Ong BC, Irrgang JJ, Fu FH, Harner CD. Clinical outcomes after isolated arthroscopic single-bundle posterior cruciate ligament reconstruction. Arthroscopy. 2005. 21(9):1042–1050.
Article20. McAllister DR, Markolf KL, Oakes DA, Young CR, McWilliams J. A biomechanical comparison of tibial inlay and tibial tunnel posterior cruciate ligament reconstruction techniques: graft pretension and knee laxity. Am J Sports Med. 2002. 30(3):312–317.
Article21. Margheritini F, Mauro CS, Rihn JA, Stabile KJ, Woo SL, Harner CD. Biomechanical comparison of tibial inlay versus transtibial techniques for posterior cruciate ligament reconstruction: analysis of knee kinematics and graft in situ forces. Am J Sports Med. 2004. 32(3):587–593.
Article22. Oakes DA, Markolf KL, McWilliams J, Young CR, McAllister DR. Biomechanical comparison of tibial inlay and tibial tunnel techniques for reconstruction of the posterior cruciate ligament: analysis of graft forces. J Bone Joint Surg Am. 2002. 84(6):938–944.
Article23. Cross MJ, Powell JF. Long-term followup of posterior cruciate ligament rupture: a study of 116 cases. Am J Sports Med. 1984. 12(4):292–297.
Article24. Hughston JC, Bowden JA, Andrews JR, Norwood LA. Acute tears of the posterior cruciate ligament: results of operative treatment. J Bone Joint Surg Am. 1980. 62(3):438–450.
Article25. Lipscomb AB Jr, Anderson AF, Norwig ED, Hovis WD, Brown DL. Isolated posterior cruciate ligament reconstruction: long-term results. Am J Sports Med. 1993. 21(4):490–496.
Article26. Schulte KR, Chu ET, Fu FH. Arthroscopic posterior cruciate ligament reconstruction. Clin Sports Med. 1997. 16(1):145–156.
Article27. Garofalo R, Jolles BM, Moretti B, Siegrist O. Double-bundle transtibial posterior cruciate ligament reconstruction with a tendon-patellar bone-semitendinosus tendon autograft: clinical results with a minimum of 2 years' follow-up. Arthroscopy. 2006. 22(12):1331–1338.
Article28. Hatayama K, Higuchi H, Kimura M, Kobayashi Y, Asagumo H, Takagishi K. A comparison of arthroscopic single- and double-bundle posterior cruciate ligament reconstruction: review of 20 cases. Am J Orthop (Belle Mead NJ). 2006. 35(12):568–571.29. Wang CJ, Weng LH, Hsu CC, Chan YS. Arthroscopic single-versus double-bundle posterior cruciate ligament reconstructions using hamstring autograft. Injury. 2004. 35(12):1293–1299.
Article30. Bergfeld JA, Graham SM, Parker RD, Valdevit AD, Kambic HE. A biomechanical comparison of posterior cruciate ligament reconstructions using single- and double-bundle tibial inlay techniques. Am J Sports Med. 2005. 33(7):976–981.
Article31. Whiddon DR, Zehms CT, Miller MD, Quinby JS, Montgomery SL, Sekiya JK. Double compared with single-bundle open inlay posterior cruciate ligament reconstruction in a cadaver model. J Bone Joint Surg Am. 2008. 90(9):1820–1829.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Bundle Anterior Cruciate Ligament Reconstruction
- Compression of the Popliteal Artery after Posterior Cruciate Ligament Reconstruction Using the Tibial Inlay Technique
- Bilateral Medial Tibial Plateau Fracture after Arthroscopic Anterior Cruciate Ligament Reconstruction
- Current Trends in Anterior Cruciate Ligament Reconstruction
- Clinical and Radiologic Results of Transtibial Single Bundle Reconstruction and Double Bundle Reconstruction of the Posterior Cruciate Ligament Using the Allo-achilles Tendon
