Clin Orthop Surg.
2011 Jun;3(2):152-156. 10.4055/cios.2011.3.2.152.
Ganglionectomy without Repairing the Bursal Defect: Long-term Results in a Series of 124 Wrist Ganglia
- Affiliations
-
- 1Department of Orthopaedic Surgery, Amalia Fleming General Hospital, Athens, Greece.
- 2Department of Anatomy, University Hospital of Alexandroupolis, Alexandroupolis, Greece. stkapetanakis@yahoo.gr
- 3Department of Orthopaedic Surgery, University Hospital of Alexandroupolis, Alexandroupolis, Greece.
- KMID: 1719313
- DOI: http://doi.org/10.4055/cios.2011.3.2.152
Abstract
- BACKGROUND
Some surgeons consider the abscission of a part of the articular bursa around the point of the input of ganglion's nape (average 1-2 cm diameter) to be very important with excellent results. However, a literature search revealed disagreement as to whether it is essential to repair a bursa defect. This study examined the effectiveness of this method without repairing the articular defect. An attempt was made to identify the anatomical origin of wrist ganglia during the surgical procedure.
METHODS
This study evaluated 124 wrist ganglia that had been treated surgically during 2004-2009 using this technique and without repairing the bursa defect (1-2 cm in diameter). The variables studied were age, gender, time from the occurrence till abscission of the ganglia, former surgical interventions, preoperative and postoperative pain, insertion of the ganglion's nape and complications. Sixty-six patients with a mean follow-up of 42 months and minimum 12 months were examined.
RESULTS
At the time of the follow-up, 80.3% had no pain whereas 92.2% showed a remarkable improvement. Seven cases of recurrence (10.6%) were found 2 to 85 months after surgery, of which most appeared during the first year (71.4%). It is important to mention that the majority of the dorsal ganglia (42.8%) originated from the capitate-lunate joint. None of the patients presented with scapholunate or other instability.
CONCLUSIONS
This surgical method is a simple and safe with excellent long-term results and a lower recurrence rate compared to other surgical approaches. Overall, repair of the articular bursa is unnecessary.
Keyword
MeSH Terms
Figure
-
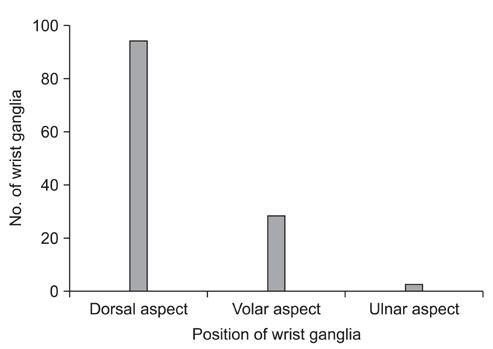
Fig. 1 Origin of ganglia.
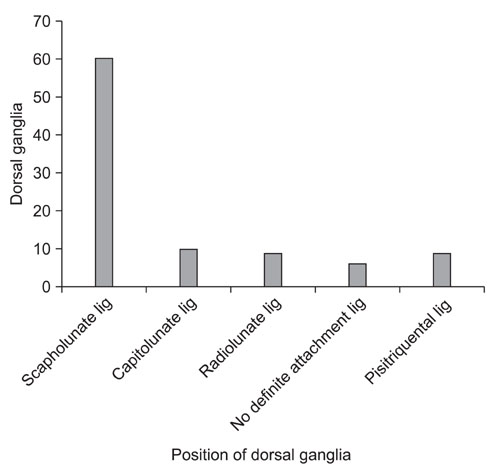
Fig. 2 Origin of dorsal ganglia. Lig: ligament.
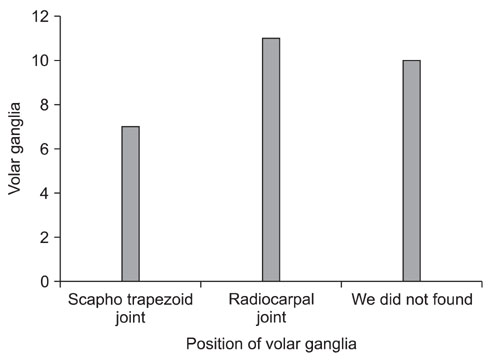
Fig. 3 Origin of volar ganglia.
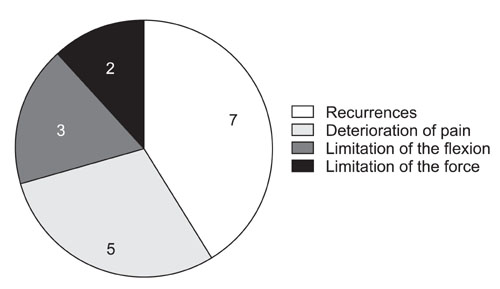
Fig. 4 Number of complications.
Reference
-
1. Bain GI, Munt J, Turner PC. New advances in wrist arthroscopy. Arthroscopy. 2008. 24(3):355–367.
Article2. McEvedy BV. The simple ganglion: a review of modes of treatment and an explanation of the frequent failures of surgery. Lancet. 1954. 266(6803):135–136.3. Osterman AL, Raphael J. Arthroscopic resection of dorsal ganglion of the wrist. Hand Clin. 1995. 11(1):7–12.
Article4. Angelides AC, Wallace PF. The dorsal ganglion of the wrist: its pathogenesis, gross and microscopic anatomy, and surgical treatment. J Hand Surg Am. 1976. 1(3):228–235.
Article5. Varley GW, Needoff M, Davis TR, Clay NR. Conservative management of wrist ganglia: aspiration versus steroid infiltration. J Hand Surg Br. 1997. 22(5):636–637.6. Holm PC, Pandey SD. Treatment of ganglia of the hand and wrist with aspiration and injection of hydrocortisone. Hand. 1973. 5(1):63–68.
Article7. Razemon JP. Surgical treatment of ganglions of the wrist by partial excision of the joint capsule: report on 303 cases. Ann Chir Main. 1983. 2(3):230–243.8. Nelson CL, Sawmiller S, Phalen GS. Ganglions of the wrist and hand. J Bone Joint Surg Am. 1972. 54(7):1459–1464.
Article9. Clay NR, Clement DA. The treatment of dorsal wrist ganglia by radical excision. J Hand Surg Br. 1988. 13(2):187–191.
Article10. Gundes H, Cirpici Y, Sarlak A, Muezzinoglu S. Prognosis of wrist ganglion operations. Acta Orthop Belg. 2000. 66(4):363–367.11. Carp L, Staut AP. A study of ganglion with special reference to treatment. Surg Gynecol Obstet. 1928. 47:460–468.12. Andren L, Eiken O. Arthrographic studies of wrist ganglions. J Bone Joint Surg Am. 1971. 53(2):299–302.
Article13. Watson HK, Rogers WD, Ashmead D 4th. Reevaluation of the cause of the wrist ganglion. J Hand Surg Am. 1989. 14(5):812–817.
Article14. Ruby LK, An KN, Linscheid RL, Cooney WP 3rd, Chao EY. The effect of scapholunate ligament section on scapholunate motion. J Hand Surg Am. 1987. 12(5 Pt 1):767–771.
Article15. Wright TW, Cooney WP, Ilstrup DM. Anterior wrist ganglion. J Hand Surg Am. 1994. 19(6):954–958.
Article16. Bienz T, Raphael JS. Arthroscopic resection of the dorsal ganglia of the wrist. Hand Clin. 1999. 15(3):429–434.
Article17. Dumontier C, Chaumeil G, Chassat R, Nourissat G. Arthroscopic treatment of dorsal wrist ganglia. Chir Main. 2006. 25:Suppl 1. S214–S220.18. Mathoulin C, Hoyos A, Pelaez J. Arthroscopic resection of wrist ganglia. Hand Surg. 2004. 9(2):159–164.
Article19. Mathoulin C, Massarella M. Therapeutic interest of wrist arthroscopy: about 1000 cases. Chir Main. 2006. 25:Suppl 1. S145–S160.20. Rocchi L, Canal A, Fanfani F, Catalano F. Articular ganglia of the volar aspect of the wrist: arthroscopic resection compared with open excision. A prospective randomised study. Scand J Plast Reconstr Surg Hand Surg. 2008. 42(5):253–259.
Article21. Aydin A, Kabakas F, Erer M, Ozkan T, Tuncer S. Surgical treatment of volar wrist ganglia. Acta Orthop Traumatol Turc. 2003. 37(4):309–312.22. Petricig P, Pepe E. First choice treatment of the pediatric wrist ganglia. Minerva Pediatr. 2006. 58(4):379–383.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The effects of superior cervical ganglionectomy on the ability of spatial memory using radial arm maze in the rats
- Left Thoracic Sympathetic Ganglionectomy with Thoracoscope for the Treatment of the Long QT Syndrome: A case report
- Intratendinous Ganglion: A Case Report
- Thoracoscopic Stellate Ganglionectomy for Facial Hyperhidrosis
- Dosal Root Ganglionectomy for a Post-Herpetic Neuralgia: Case Report
