Arthroscopic Percutaneous Repair of Anterosuperior Rotator Cuff Tear Including Biceps Long Head: A 2-Year Follow-up
- Affiliations
-
- 1Department of Orthopaedic Surgery, Hallym University College of Medicine, Chuncheon, Korea. ybw1999@gmail.com
- KMID: 1719296
- DOI: http://doi.org/10.4055/cios.2012.4.4.284
Abstract
- BACKGROUND
To report the results of an arthroscopic percutaneous repair technique for partial-thickness tears of the anterosuperior cuff combined with a biceps lesion.
METHODS
The inclusion criteria were evidence of the upper subscapularis tendon tear and an articular side partial-thickness tear of the supraspinatus tendon, degeneration of the biceps long head or degenerative superior labrum anterior-posterior, above lesions treated by arthroscopic percutaneous repair, and follow-up duration > 24 months after the operation. American Shoulder and Elbow Surgeons (ASES) score, constant score, the pain level on a visual analogue scale, ranges of motion and strength were assessed.
RESULTS
The mean (+/- standard deviation) age of the 20 enrolled patients was 56.0 +/- 7.7 years. The forward flexion strength increased from 26.3 +/- 6.7 Nm preoperatively to 38.9 +/- 5.1 Nm at final follow-up. External and internal rotation strength was also significantly increased (14.2 +/- 1.7 to 19.1 +/- 3.03 Nm, 12.3 +/- 3.2 to 18.1 +/- 2.8 Nm, respectively). Significant improvement was observed in ASES and constant scores at 3 months, 1 year and the time of final follow-up when compared with preoperative scores (p < 0.001). The mean subjective shoulder value was 86% (range, 78% to 97%).
CONCLUSIONS
The implementation of complete rotator cuff repair with concomitant tenodesis of the biceps long head using arthroscopic percutaneous repair achieved full recovery of normal rotator cuff function, maximum therapeutic efficacy, and patient satisfaction.
MeSH Terms
Figure
-
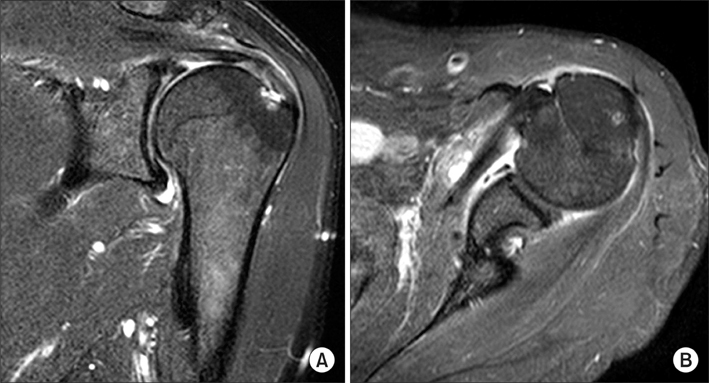
Fig. 1 Conventional magnetic resonance imaging with T2-weighted images in the oblique coronal and axial planes show partial tear of supraspinatus tendon (A) and subscapularis tendon (B). The disrupted transverse ligament covering the bicipital groove was noted.

Fig. 2 The procedure for subscapularis tendon repair. (A) 3.7 mm punch for a suture anchor at the footprint of the subscapularis tendon. (B) Polydioxanone monofilament absorbable suture passed through the spinal needle and substance of the subscapularis tendon. (C) FiberWire suture limbs of the anchor passed through the subscapularis tendon. (D) The subscapularis tendon securely fixed to its insertion site and its tension restored.
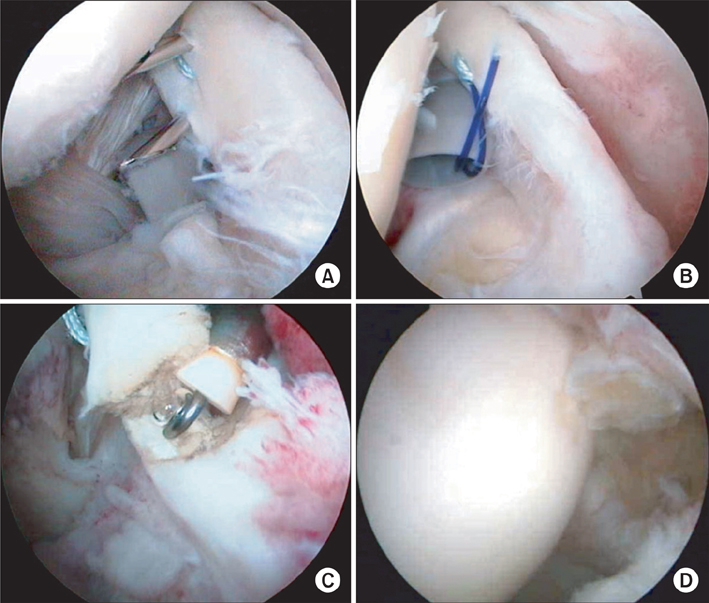
Fig. 3 (A, B) Introduction of 18-G spinal needles through the biceps tendon through most of the superolateral rotator interval tissue followed by passing the polydioxanone suture through the 18-G needles to switch to FiberWire suture. (C) The root of the biceps long head cut by an electrocautery device through the anterior portal. (D) Intra-articular view after biceps tenodesis using the percutaneous intra-articular transtendon technique.

Fig. 4 (A) The polydioxanone suture passing through each of the 18-G spinal needles to exchange it into a loaded suture on the anchor following the insertion of 3.7 mm suture tak anchor at the far medial edge of the footprint at a dead man's angle of 45° or less. (B) Intra-articular view after complete repair of the partial articular side tear of suparaspinatus tendon lesion.
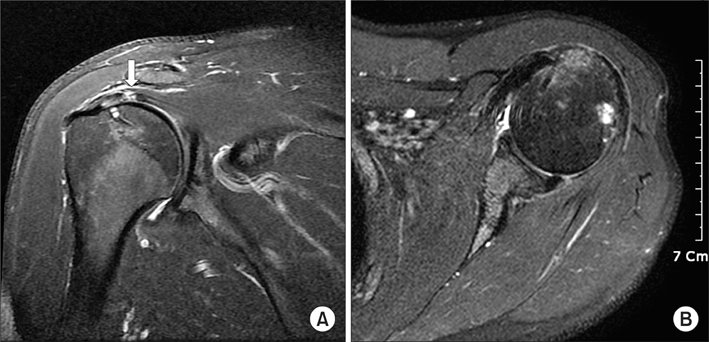
Fig. 5 (A) Follow-up magnetic resonance imaging taken at 2 years indicates incomplete healing defect (arrow) of supraspatus tendon. (B) Subscapularis tendon that was simultaneously repaired shows complete integrity. The 4 of 11 patients had an evident partial thickness defect under supraspinatus tendon that was initially fixed, but no correlation with clinical outcome.
Reference
-
1. Fox J, Romeo AA. Arthroscopic subscapularis repair. In : Annual Meeting of the American Academy of Orthopaedic Surgeons; 2003 Feb 5-9; New Orleans, LA, USA.2. Lafosse L, Jost B, Reiland Y, Audebert S, Toussaint B, Gobezie R. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J Bone Joint Surg Am. 2007. 89(6):1184–1193.
Article3. Arai R, Sugaya H, Mochizuki T, Nimura A, Moriishi J, Akita K. Subscapularis tendon tear: an anatomic and clinical investigation. Arthroscopy. 2008. 24(9):997–1004.
Article4. Burkhart SS, Tehrany AM. Arthroscopic subscapularis tendon repair: technique and preliminary results. Arthroscopy. 2002. 18(5):454–463.5. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF. Traumatic tears of the subscapularis tendon: clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med. 1997. 25(1):13–22.6. Gerber C, Hersche O, Farron A. Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am. 1996. 78(7):1015–1023.7. Ide J, Tokiyoshi A, Hirose J, Mizuta H. Arthroscopic repair of traumatic combined rotator cuff tears involving the subscapularis tendon. J Bone Joint Surg Am. 2007. 89(11):2378–2388.
Article8. Pfirrmann CW, Zanetti M, Weishaupt D, Gerber C, Hodler J. Subscapularis tendon tears: detection and grading at MR arthrography. Radiology. 1999. 213(3):709–714.
Article9. Smith JG. The classic: pathological appearances of seven cases of injury of the shoulder-joint: with remarks 1834. Clin Orthop Relat Res. 2010. 468(6):1471–1475.
Article10. Gerber C, Sebesta A. Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: a preliminary report. J Shoulder Elbow Surg. 2000. 9(6):483–490.
Article11. Habermeyer P, Magosch P, Pritsch M, Scheibel MT, Lichtenberg S. Anterosuperior impingement of the shoulder as a result of pulley lesions: a prospective arthroscopic study. J Shoulder Elbow Surg. 2004. 13(1):5–12.
Article12. Nho SJ, Frank RM, Reiff SN, Verma NN, Romeo AA. Arthroscopic repair of anterosuperior rotator cuff tears combined with open biceps tenodesis. Arthroscopy. 2010. 26(12):1667–1674.
Article13. Boileau P, Krishnan SG, Coste JS, Walch G. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002. 18(9):1002–1012.
Article14. Lo IK, Burkhart SS. Transtendon arthroscopic repair of partial-thickness, articular surface tears of the rotator cuff. Arthroscopy. 2004. 20(2):214–220.
Article15. Lopez-Vidriero E, Costic RS, Fu FH, Rodosky MW. Biomechanical evaluation of 2 arthroscopic biceps tenodeses: double-anchor versus percutaneous intra-articular transtendon (PITT) techniques. Am J Sports Med. 2010. 38(1):146–152.
Article16. Sekiya JK, Elkousy HA, Rodosky MW. Arthroscopic biceps tenodesis using the percutaneous intra-articular transtendon technique. Arthroscopy. 2003. 19(10):1137–1141.
Article17. Flury MP, John M, Goldhahn J, Schwyzer HK, Simmen BR. Rupture of the subscapularis tendon (isolated or in combination with supraspinatus tear): when is a repair indicated? J Shoulder Elbow Surg. 2006. 15(6):659–664.
Article18. Waibl B, Buess E. Partial-thickness articular surface supraspinatus tears: a new transtendon suture technique. Arthroscopy. 2005. 21(3):376–381.
Article19. Bennett WF. Arthroscopic repair of anterosuperior (supraspinatus/subscapularis) rotator cuff tears: a prospective cohort with 2- to 4-year follow-up. Classification of biceps subluxation/instability. Arthroscopy. 2003. 19(1):21–33.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Medial Dislocation of the Long Head of the Biceps without Rotator Cuff Tear: A Case Report
- Arthroscopic repair of large and massive rotator cuff tears—“sandwich augmentation” with the long head of the biceps tendon: a technical note
- Arthroscopic Changes of the Biceps Pulley in Rotator Cuff Tear and Its Clinical Significance in Relation to Treatment
- Mid-term Results of Biceps Incorporating Suture Without Deteaching the Biceps Tendon from the Flenoid in the Large or Massive Cuff Tear
- Treatment of Massive Rotator Cuff Tears: Focusing on Arthroscopic Approach
