A Case of Acute Esophageal Necrosis with Gastric Outlet Obstruction
- Affiliations
-
- 1Departmemt of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. ikkim1003@hanmail.net
- KMID: 1718373
- DOI: http://doi.org/10.4166/kjg.2010.56.5.314
Abstract
- Acute esophageal necrosis (AEN) is a very rare disorder typically presenting as a diffuse black esophageal mucosa on upper endoscopy. For this reason, AEN is often considered to be synonymous with 'black esophagus'. The pathogenesis of entity is still unknown. We report a case of AEN with duodenal ulcer causing partial gastric outlet obstruction. A 53-year-old man presented with hematemesis after repeated vomiting. The upper gastrointestinal endoscopy revealed circumferential black coloration on middle 315 to lower esophageal mucosa that stopped abruptly at the gastroesophageal junction. Pyloric ring deformity and active duodenal ulceration with extensive edema was observed. After conservative management with NPO and intravenous proton pump inhibitor, he showed clinical and endoscopic improvement. He resumed an oral diet on day 7 and was discharged. In our case the main pathogenesis of disease could be accounted for massive esophageal reflux due to transient gastric outlet obstruction by duodenal ulcer and following local ischemic injury.
MeSH Terms
-
Acute Disease
Duodenal Ulcer/drug therapy/etiology
Endoscopy, Gastrointestinal
Esophageal Diseases/complications/*diagnosis/drug therapy
Esophagus/*pathology
Gastric Outlet Obstruction/*complications/pathology
Humans
Ischemia/pathology
Male
Middle Aged
Necrosis
Proton Pump Inhibitors/therapeutic use
Tomography, X-Ray Computed
Figure
-

Fig. 1. Endoscopic images of case. Black colored esophageal mucosa was noted through middle to lower esophagus (A) that ended sharply at gastroesophageal junction. (B) Extensive ulceration and edematous mucosa was also noted.

Fig. 2. CT image of case. Deep ulceration at pylorus and duodenal bulb area caused the deformity and stricture of gastric outlet.
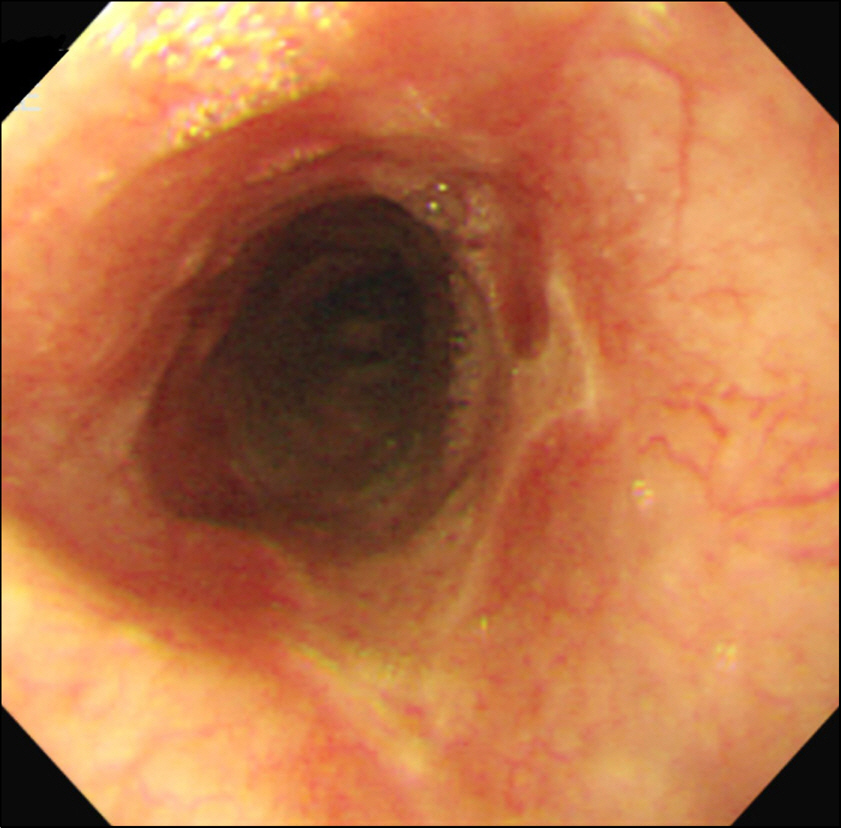
Fig. 3. Follow up endoscopic image. Shallow ulceration with whitish exudates substituted previous black pigmented esophageal mucosa. 6 days after the restriction of oral feeding and intravenous administration of proton pump inhibitor.
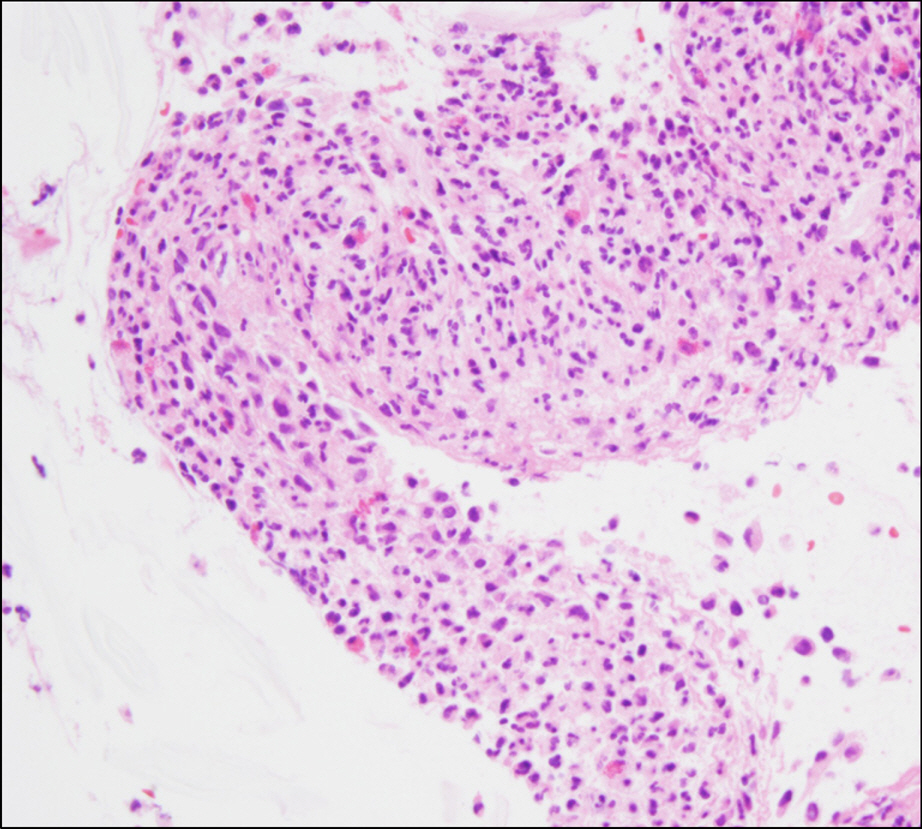
Fig. 4. Microscopic findings of esophageal mucosa. Biopsy which was performed at follow up endoscopy showed inflammatory exudates and inflammatory granulation tissue including apoptotic cells and regenerating cells (H&E stain, ×400).
Reference
-
1. Hong J, Kim S, Park H, Seo J, Lee Y, Kim H. Black esophagus associated with alcohol abuse. Gut Liver. 2008; 2:133–135.
Article2. Goldenberg SP, Wain SL, Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990; 98:493–496.
Article3. Etienne JP, Roge J, Delavierre P, Veyssier P. Esophageal necrosis of vascular origin. Sem Hop. 1969; 45:1599–1606.4. Moretó M, Ojembarrena E, Zaballa M, Tá nago JG, Ibá nez S. Idiopathic acute esophageal necrosis: not necessarily a terminal event. Endoscopy. 1993; 25:534–538.
Article5. Augusto F, Fernandes V, Cremers MI, et al. Acute necrotizing esophagitis: a large retrospective case series. Endoscopy. 2004; 36:411–415.
Article6. Aharinejad S, Lametschwandtner A, Franz P, Firbas W. The vascularization of the digestive tract studied by scanning elec-tron microscopy with special emphasis on the teeth, esophagus, stomach, small and large intestine, pancreas, and liver. Scanning Microsc. 1991; 5:811–849.7. Ben Soussan E, Savoye G, Hochain P, et al. Acute esophageal necrosis: a 1-year prospective study. Gastrointest Endosc. 2002; 56:213–217.8. Lacy BE, Toor A, Bensen SP, Rothstein RI, Maheshwari Y. Acute esophageal necrosis: report of two cases and a review of the literature. Gastrointest Endosc. 1999; 49:527–532.
Article9. Endo T, Sakamoto J, Sato K, et al. Acute esophageal necrosis caused by alcohol abuse. World J Gastroenterol. 2005; 11:5568–5570.
Article10. Reichart M, Busch OR, Bruno MJ, Van Lanschot JJ. Black esophagus: a view in the dark. Dis Esophagus. 2000; 13:311–313.
Article11. Grudell AB, Mueller PS, Viggiano TR. Black esophagus: report of six cases and review of the literature, 1963-2003. Dis Esophagus. 2006; 19:105–110.
Article12. Orlando RC, Powell DW, Carney CN. Pathophysiology of acute acid injury in rabbit esophageal epithelium. J Clin Invest. 1981; 68:286–293.
Article13. Tobey NA, Orlando RC. Mechanisms of acid injury to rabbit esophageal epithelium. Role of basolateral cell membrane acidification. Gastroenterology. 1991; 101:1220–1228.14. Bass BL, Schweitzer EJ, Harmon JW, Kraimer J. H+ back diffusion interferes with intrinsic reactive regulation of esophageal mucosal blood flow. Surgery. 1984; 96:404–413.15. Barjas E, Pires S, Lopes J, et al. Cytomegalovirus acute necrotizing esophagitis. Endoscopy. 2001; 33:735.
Article16. Cattan P, Cuillerier E, Cellier C, et al. Black esophagus associated with herpes esophagitis. Gastrointest Endosc. 1999; 49:105–107.
Article17. Katsinelos P, Pilpilidis I, Dimiropoulos S, et al. Black esophagus induced by severe vomiting in a healthy young man. Surg Endosc. 2003; 17:521.
Article18. Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: a rare syndrome. J Gastroenterol. 2007; 42:29–38.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Man with Dysphagia after Cervical Esophagogastrostomy: A Case Report
- Acute Gastric Necrosis Due to Gastric Outlet Obstruction Accompanied with Gastric Cancer and Trichophytobezoar
- A Case of Congenital Gastric Outlet Obstruction with Serosal Fibrous Band in Prematurity
- A Case Report of Gastric Dilatation
- A Case of Aggravated Esophageal Candidiasis and Gastric Yeast Bezoar Formation following Gastric Outlet Obstruction due to Duodenal Stenosis
