Korean J Gastroenterol.
2010 Feb;55(2):100-108. 10.4166/kjg.2010.55.2.100.
Clinical Analysis of Recurrence Rate and Symptom Improvement in Gastro-esophageal Reflux Disease Patients
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. dhljohn@snubh.org
- 2Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1718293
- DOI: http://doi.org/10.4166/kjg.2010.55.2.100
Abstract
- BACKGROUND/AIMS
Gastro-esophageal reflux disease (GERD) is a chronic condition, with 50-80% of patients experiencing recurrence within one year following completion of initial treatment. The present study aimed to estimate recurrence rate and treatment response in GERD patients treated with proton pump inhibitor.
METHODS
A total of 207 symptomatic GERD patients, which were confirmed by endoscopy from July 2008 till January 2009, were enrolled. They were divided into non-erosive reflux disease (NERD) group and erosive reflux disease (ERD) group by endoscopic findings. Patients were treated with lansoprazole 15 mg (NERD group) or 30 mg (ERD group) once daily for 8 weeks. The presence of symptoms was assessed in each patient at baseline and post-treatment using a questionnaire. Subsequent symptomatic recurrence on the cessation of therapy in each improved patients was checked by telephone survey or outpatient interview.
RESULTS
Ninety-four patients and 113 patients were first diagnosed with NERD and ERD, respectively. The mean post-treatment follow-up period was 24.4+/-8.5 weeks. Recurrence rate was 40.0% (NERD, 43.8%; ERD, 37.1% (p=0.224)). Recurrence time was 10.1+/-5.8 weeks (NERD 9.6 weeks; ERD, 10.6 weeks (p=0.444)). Regarding the symptom improvement after 8 week therapy with lansoprazole, 89.4% (NERD, 85.1%; ERD, 92.9% (p=0.056)) of total patients were symptomatically improved.
CONCLUSIONS
Forty percentage of GERD patients recurred within 6 months following the completion of 8 week therapy with lansoprazole. Recurrence rate, recurrence time, and rate of symptom improvement were not significantly different between NERD group treated with half dose and ERD group treated with full dose lansoprazole.
MeSH Terms
Figure
-
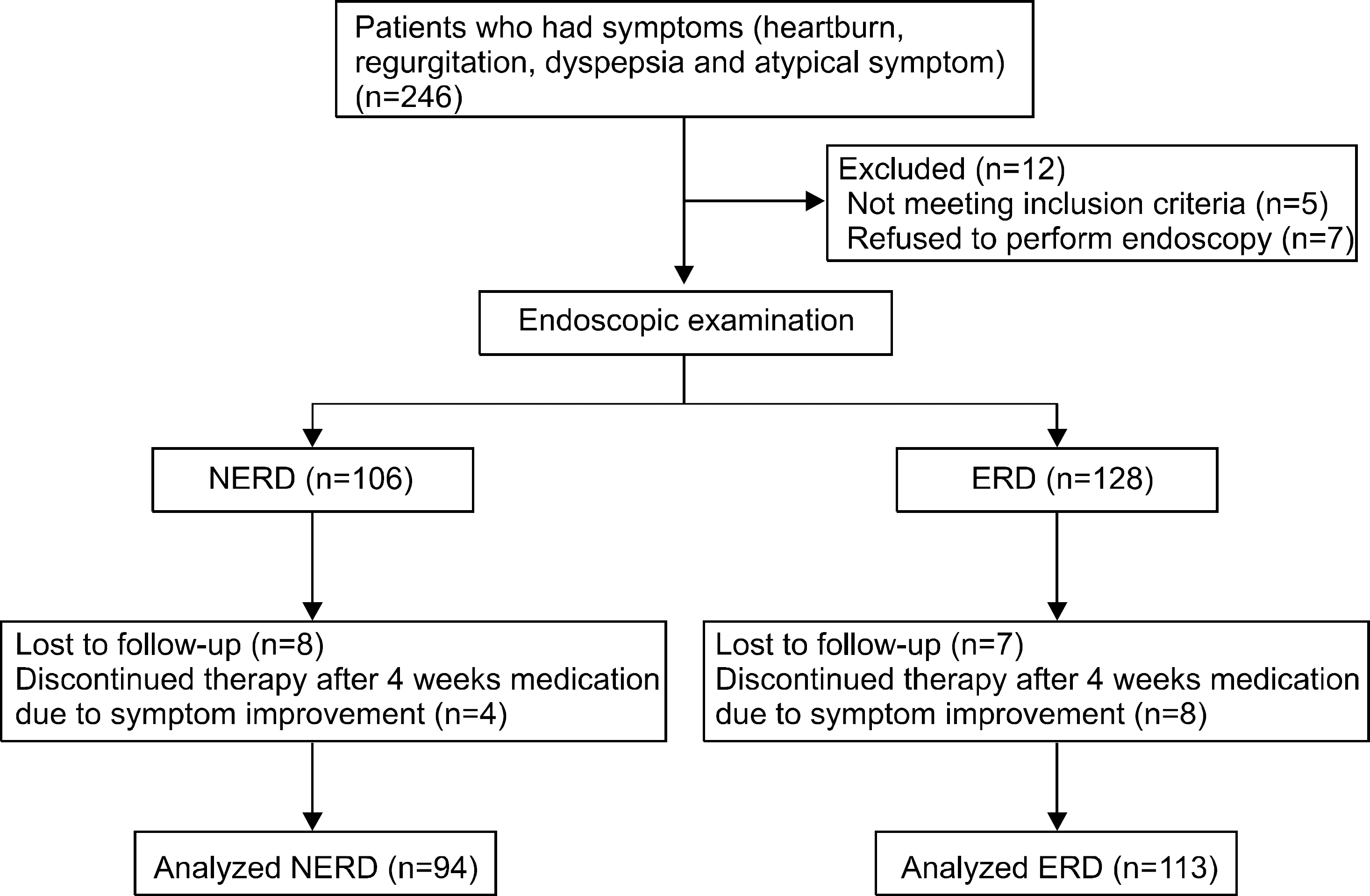
Fig. 1. Algorithm of study protocol in symptomatic GERD patients. NERD, nonerosive reflux disease; ERD, erosive reflux disease.
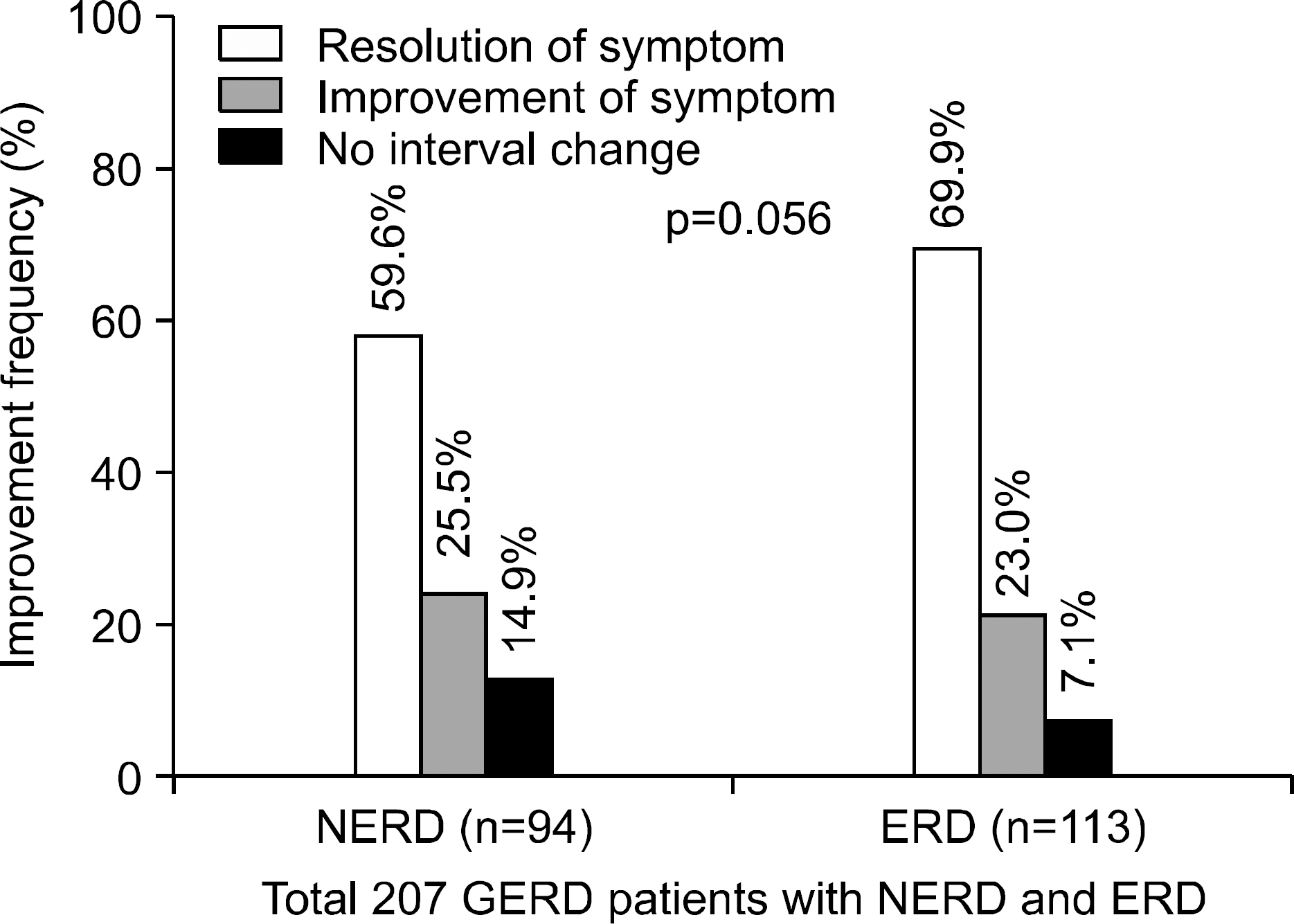
Fig. 2. Treatment outcome among 207 GERD patients with NERD and ERD. NERD, nonerosive reflux disease; ERD, erosive reflux disease.
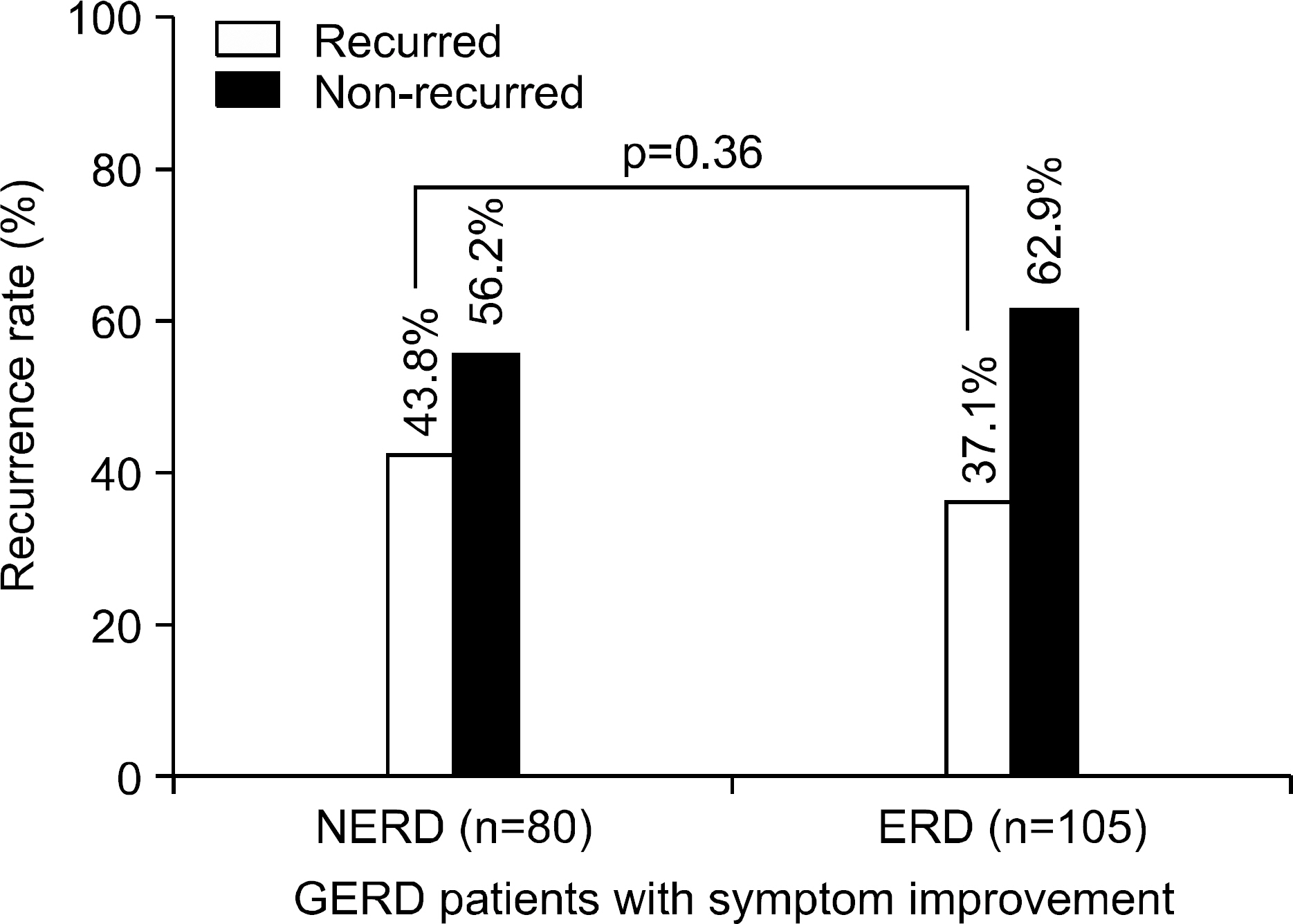
Fig. 3. Recurrence rate in GERD patients with symptom improvement after PPI treatment. NERD, nonerosive reflux disease; ERD, erosive reflux disease.
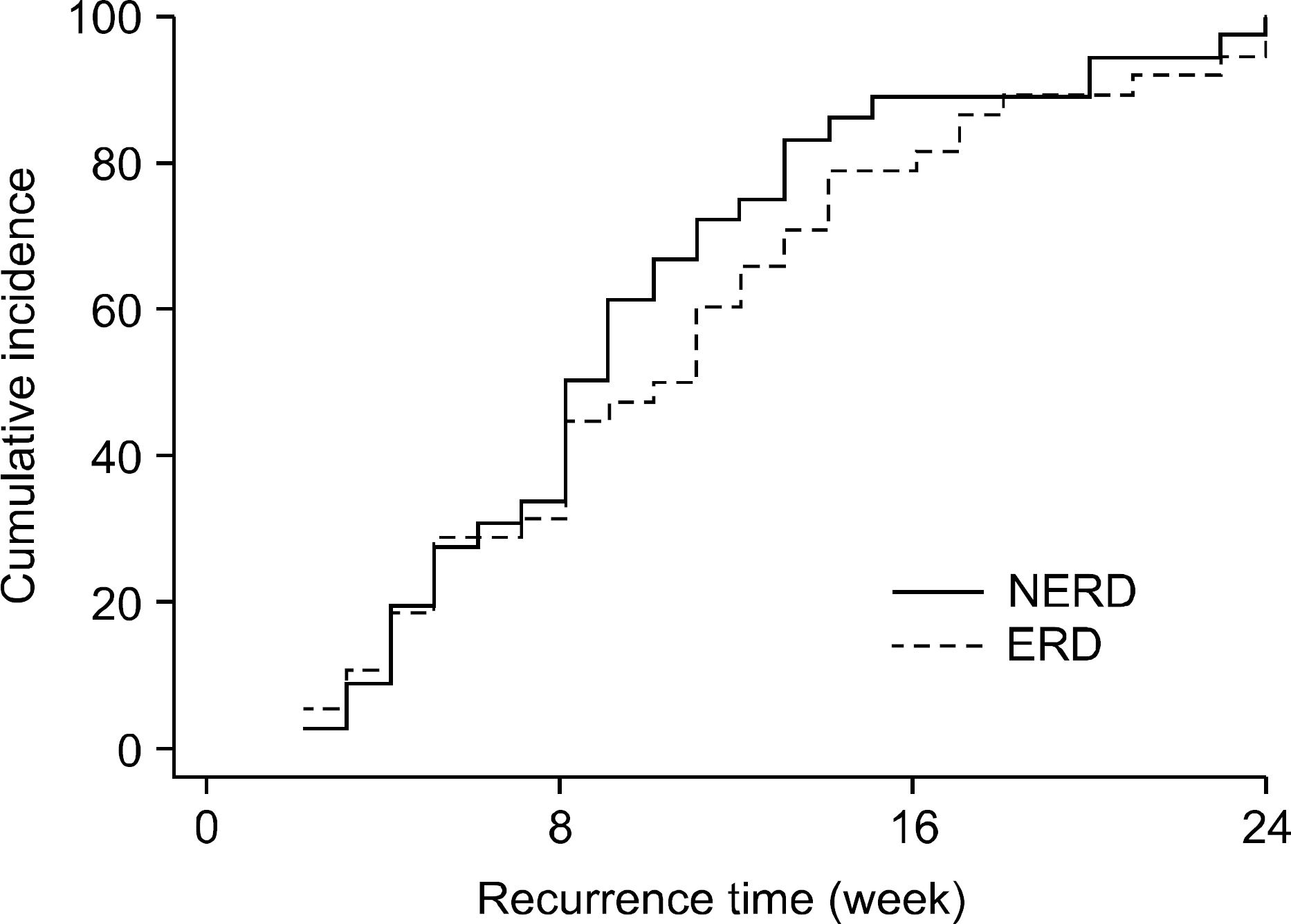
Fig. 4. Recurrence time by Kaplan-Meier Method and Log Rank comparisons of the NERD (n=35) and ERD (n=39) group. NERD, nonerosive reflux disease; ERD, erosive reflux disease.
Reference
-
1. Richter JE. The many manifestations of gastroesophageal reflux disease: presentation, evaluation, and treatment. Gastroenterol Clin North Am. 2007; 36:577–599. viii-ix.
Article2. Heading RC. Prevalence of upper gastrointestinal symptoms in the general population: a systematic review. Scand J Gastroenterol. 1999; 231(suppl):S3–S8.3. Locke GR 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ 3rd. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minne-sota. Gastroenterology. 1997; 112:1448–1456.
Article4. Yoo SS, Lee WH, Ha J, et al. The prevalence of esophageal disorders in the subjects examined for health screening. Korean J Gastroenterol. 2007; 50:306–312.5. Hwang JK, Kim J, Hong SG, et al. A prospective multicenter study on the prevalence and symptoms of erosive reflux esophagitis in secondary and tertiary hospitals in Korea. Korean J Gastroenterol. 2009; 53:283–291.
Article6. Jaspersen D. Extraesophageal disorders in gastroesophageal reflux disease. Dig Dis. 2004; 22:115–119.
Article7. Martinez-Serna T, Tercero F Jr, Filipi CJ, et al. Symptom priority ranking in the care of gastroesophageal reflux: a review of 1,850 cases. Dig Dis. 1999; 17:219–224.
Article8. Shapiro M, Green C, Faybush EM, Esquivel RF, Fass R. The extent of oesophageal acid exposure overlap among the different gastro-oesophageal reflux disease groups. Aliment Pharmacol Ther. 2006; 23:321–329.
Article9. Dent J. Gastro-oesophageal reflux disease. Digestion. 1998; 59:433–445.
Article10. Martinez SD, Malagon IB, Garewal HS, Cui H, Fass R. Non-erosive reflux disease (NERD)–acid reflux and symptom patterns. Aliment Pharmacol Ther. 2003; 17:537–545.11. Fass R. Erosive esophagitis and nonerosive reflux disease (NERD): comparison of epidemiologic, physiologic, and therapeutic characteristics. J Clin Gastroenterol. 2007; 41:131–137.12. Moayyedi P, Talley NJ. Gastro-oesophageal reflux disease. Lancet. 2006; 367:2086–2100.
Article13. McDougall NI, Johnston BT, Kee F, Collins JS, McFarland RJ, Love AH. Natural history of reflux oesophagitis: a 10 year follow up of its effect on patient symptomatology and quality of life. Gut. 1996; 38:481–486.
Article14. Olbe L, Lundell L. Medical treatment of reflux esophagitis. Hepatogastroenterology. 1992; 39:322–324.15. Freston JW, Malagelada JR, Petersen H, McCloy RF. Critical issues in the management of gastroesophageal reflux disease. Eur J Gastroenterol Hepatol. 1995; 7:577–586.16. Donnellan C, Sharma N, Preston C, Moayyedi P. Medical treatments for the maintenance therapy of reflux oesophagitis and endoscopic negative reflux disease. Cochrane Database Syst Rev. 2005. CD003245.
Article17. Haruma K, Hamada H, Mihara M, et al. Negative association between Helicobacter pylori infection and reflux esophagitis in older patients: case-control study in Japan. Helicobacter. 2000; 5:24–29.18. Wu JC, Sung JJ, Ng EK, et al. Prevalence and distribution of Helicobacter pylori in gastroesophageal reflux disease: a study from the East. Am J Gastroenterol. 1999; 94:1790–1794.19. Labenz J, Blum AL, Bayerdorffer E, Meining A, Stolte M, Borsch G. Curing Helicobacter pylori infection in patients with duodenal ulcer may provoke reflux esophagitis. Gastroenterology. 1997; 112:1442–1447.20. Fallone CA, Barkun AN, Friedman G, et al. Is Helicobacter pylori eradication associated with gastroesophageal reflux disease? Am J Gastroenterol. 2000; 95:914–920.21. Laine L, Sugg J. Effect of Helicobacter pylori eradication on development of erosive esophagitis and gastroesophageal reflux disease symptoms: a post hoc analysis of eight double blind prospective studies. Am J Gastroenterol. 2002; 97:2992–2997.22. Schwizer W, Thumshirn M, Dent J, et al. Helicobacter pylori and symptomatic relapse of gastro-oesophageal reflux disease: a randomised controlled trial. Lancet. 2001; 357:1738–1742.23. Rhee PL. Association between Helicobacter pylori and gastroesophageal reflux disease. Korean J Gastroenterol. 2003; 42:179–182.24. Delaney B, McColl K. Review article: Helicobacter pylori and gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2005; 22(suppl 1):S32–S40.25. Armstrong D, Bennett JR, Blum AL, et al. The endoscopic assessment of esophagitis: a progress report on observer agreement. Gastroenterology. 1996; 111:85–92.
Article26. Hetzel DJ, Dent J, Reed WD, et al. Healing and relapse of severe peptic esophagitis after treatment with omeprazole. Gastroenterology. 1988; 95:903–912.
Article27. Caro JJ, Salas M, Ward A. Healing and relapse rates in gastroesophageal reflux disease treated with the newer proton-pump inhibitors lansoprazole, rabeprazole, and pantoprazole compared with omeprazole, ranitidine, and placebo: evi-dence from randomized clinical trials. Clin Ther. 2001; 23:998–1017.
Article28. Jee SR, Seol SY, Kim DH, et al. A randomized, comparative study of rabeprazole vs. ranitidine maintenance therapies for reflux esophagitis–multicenter study. Korean J Gastroenterol. 2005; 45:321–327.29. Tack J, Fass R. Review article: approaches to endoscopic- negative reflux disease: part of the GERD spectrum or a unique acid-related disorder? Aliment Pharmacol Ther. 2004; 19(suppl 1):S28–S34.30. Fass R, Tougas G. Functional heartburn: the stimulus, the pain, and the brain. Gut. 2002; 51:885–892.
Article31. Lee ES, Kim N, Lee SH, et al. Comparison of risk factors and clinical responses to proton pump inhibitors in patients with erosive oesophagitis and non-erosive reflux disease. Aliment Pharmacol Ther. 2009; 30:154–164.
Article32. Quigley EM. Factors that influence therapeutic outcomes in symptomatic gastroesophageal reflux disease. Am J Gastroenterol. 2003; 98(suppl):S24–S30.
Article33. Lee KJ, Kwon HC, Cheong JY, Cho SW. Demographic, clinical, and psychological characteristics of the heartburn groups classified using the Rome III criteria and factors associated with the responsiveness to proton pump inhibitors in the gastroesophageal reflux disease group. Digestion. 2009; 79:131–136.
Article34. Jaspersen D, Kulig M, Labenz J, et al. Prevalence of ex-tra-oesophageal manifestations in gastro-oesophageal reflux disease: an analysis based on the ProGERD Study. Aliment Pharmacol Ther. 2003; 17:1515–1520.
Article35. Dent J, Jones R, Kahrilas P, Talley NJ. Management of gas-tro-oesophageal reflux disease in general practice. BMJ. 2001; 322:344–347.
Article36. Dean BB, Gano AD Jr, Knight K, Ofman JJ, Fass R. Effectiveness of proton pump inhibitors in nonerosive reflux disease. Clin Gastroenterol Hepatol. 2004; 2:656–664.
Article37. Richter JE, Kahrilas PJ, Johanson J, et al. Efficacy and safety of esomeprazole compared with omeprazole in GERD patients with erosive esophagitis: a randomized controlled trial. Am J Gastroenterol. 2001; 96:656–665.
Article38. Richter JE, Bochenek W. Oral pantoprazole for erosive esophagitis: a placebo-controlled, randomized clinical trial. Pantoprazole US GERD Study Group. Am J Gastroenterol. 2000; 95:3071–3080.39. Bardhan KD, Hawkey CJ, Long RG, et al. Lansoprazole versus ranitidine for the treatment of reflux oesophagitis. UK Lansoprazole Clinical Research Group. Aliment Pharmacol Ther. 1995; 9:145–151.40. Castell DO, Richter JE, Robinson M, Sontag SJ, Haber MM. Efficacy and safety of lansoprazole in the treatment of erosive reflux esophagitis. The Lansoprazole Group. Am J Gastroenterol. 1996; 91:1749–1757.41. Sharma VK, Leontiadis GI, Howden CW. Meta-analysis of randomized controlled trials comparing standard clinical doses of omeprazole and lansoprazole in erosive oesophagitis. Aliment Pharmacol Ther. 2001; 15:227–231.
Article42. Varanasi RV, Fantry GT, Wilson KT. Decreased prevalence of Helicobacter pylori infection in gastroesophageal reflux disease. Helicobacter. 1998; 3:188–194.43. Hackelsberger A, Schultze V, Gunther T, von Arnim U, Manes G, Malfertheiner P. The prevalence of Helicobacter pylori gastritis in patients with reflux oesophagitis: a case- control study. Eur J Gastroenterol Hepatol. 1998; 10:465–468.44. Raghunath A, Hungin AP, Wooff D, Childs S. Prevalence of Helicobacter pylori in patients with gastro-oesophageal reflux disease: systematic review. BMJ. 2003; 326:737.45. Wu JC, Cheung CM, Wong VW, Sung JJ. Distinct clinical characteristics between patients with nonerosive reflux disease and those with reflux esophagitis. Clin Gastroenterol Hepatol. 2007; 5:690–695.
Article46. Kim HY, Kim NY, Kim SM, et al. Clinical spectrum and risk factors of erosive and non-erosive GERD in health check-up subjects. Korean J Med. 2006; 71:491–500.47. Labenz J, Armstrong D, Zetterstrand S, Eklund S, Leodolter A. Clinical trial: factors associated with freedom from relapse of heartburn in patients with healed reflux oesophagitis–results from the maintenance phase of the EXPO study. Aliment Pharmacol Ther. 2009; 29:1165–1171.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Esophageal Manometry and 24 Hours Ambulatory Esophageal pH Monitoring in Patients with Globus Pharyngeus
- Small Intestinal(gastro)esophageal Reflux in Different Types of Gastrectomy : 24 Hour Esophageal Bilirubin Monitoring
- Is Gastroesophageal Reflux Disease and Achalasia Coincident or Not?
- Multicenter Study to Evaluate the Effect of Esomeprozole in Gastro-esophageal Reflux Disease
- The Relationship between Ineffective Esophageal Motility and Gastro-esophageal Reflux Disease
