J Korean Med Sci.
2007 Feb;22(1):173-176. 10.3346/jkms.2007.22.1.173.
Ruptured Anterior Communicating Artery Aneurysm Causing Bilateral Oculomotor Nerve Palsy: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, School of Medicine, Institute of Wonkwang Medical Science, Wonkwang University, Iksan, Korea. kangsd@wonkwang.ac.kr
- KMID: 1713263
- DOI: http://doi.org/10.3346/jkms.2007.22.1.173
Abstract
- A rare case of bilateral third cranial nerve palsy due to a ruptured anterior communicating artery aneurysm is presented. A 68-yr-old woman was semicomatose with bilaterally fixed dilated pupil, abducted eyes, and ptosis. A computed tomography demonstrated extensive hemorrhage spreading around the both Sylvian and interhemisheric fissure without focal mass effect. Intracranial pressure via extraventricular drainage before surgery was 15-50 mmHg. Three months later, brain MRI showed infarction of left posterior cerebral artery territory and lacuna infarction of the pons. Eleven months after aneurysm repair, nerve palsy improved slowly and recovered partially. The patient communicated well with simple words. The author reviewed and discussed the possible mechanism of this rare neuro-ophthalmological manifestation in view of a false localizing sign.
MeSH Terms
Figure
-

Fig. 1 Computed tomographic scanning demonstrates extensive hemorrhage spreading around the both Sylvian, basal, and interhemispheric cistern.

Fig. 2 A digital subtraction angiogram reveals a saccular aneurysm on the anterior communicating artery.
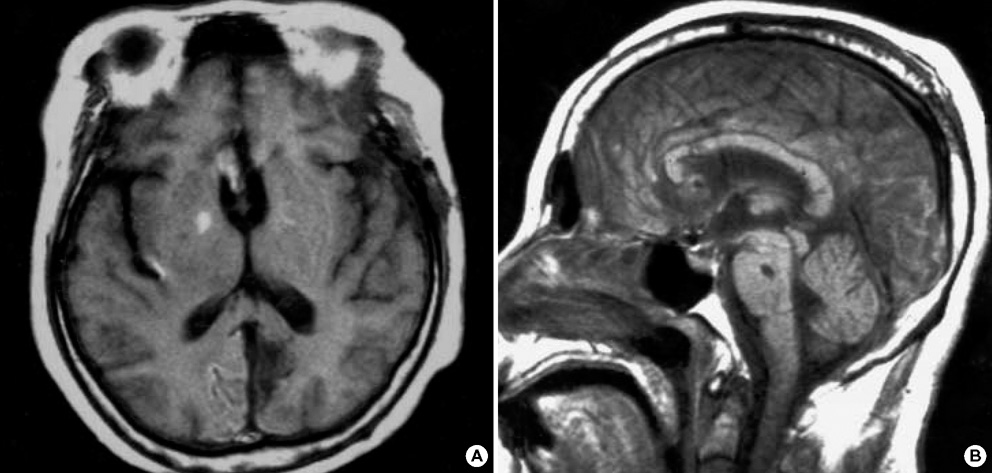
Fig. 3 Three months after surgery, a follow-up magnetic resonance imaging demonstrates infarction of the left medial occipital lobe (A) and lacunar infarction of the pons (B).
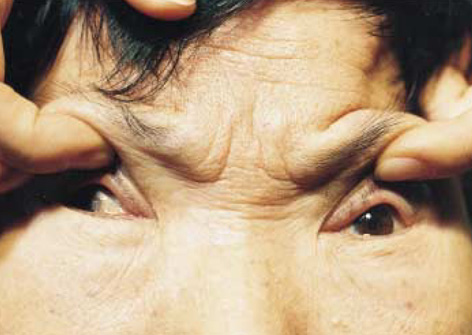
Fig. 4 Postoperative photograph by one year follow-up shows lateral deviation in the right eye, centrally fixed pupil in the left eye, and both isocoric and reactive pupils.
Reference
-
1. Lee CH, Koh YC. Ruptured posterior communicating artery aneurysm causing bilateral abducens nerve paralyses. J Korean Neurosurg Soc. 2000. 29:426–429.2. Ziyal IM, Ozcan OE, Deniz E, Bozkurt G, Ismailoglu O. Early improvement of bilateral abducens nerve palsies following surgery of an anterior communicating artery aneurysm. Acta Neurochir (Wien). 2003. 145:159–161.
Article3. Suzuki J, Iwabuchi T. Ocular motor disturbances occurring as false localizing signs in ruptured intracranial aneurysms. Acta Neurochir (Wien). 1974. 30:119–128.
Article4. Coyne TJ, Wallace MC. Bilateral third cranial nerve palsies in association with a ruptured anterior communicating artery aneurysm. Surg Neurol. 1994. 42:52–56.
Article5. Fox JL. Intracranial aneurysms. 1983. New York: Springer;163–183.6. Kudo T. Postoperative oculomotor palsy due to vasospasm in a patient with a ruptured internal carotid artery aneurysm: a case report. Neurosurgery. 1986. 19:274–277.
Article7. Trobe JD. Isolated third nerve palsies. Semin Neurol. 1986. 6:135–141.
Article8. Trobe JD. Third nerve palsy and the pupil. Footnotes to the rule. Arch Ophthalmol. 1988. 106:601–602.9. Good EF. Ptosis as the sole manifestation of compression of the oculomotor nerve by an aneurysm of the posterior communicating artery. J Clin Neuroophthalmol. 1990. 10:59–61.10. Kissel JT, Burde RM, Klingele TG, Zeiger HE. Pupil-sparing oculomotor palsies with internal carotid-posterior communicating artery aneurysms. Ann Neurol. 1983. 13:149–154.
Article11. Terry JE, Stout T. A pupil-sparing oculomotor palsy from a contralateral giant intracavernous aneurysm. J Am Optom Assoc. 1990. 61:640–645.12. Asbury AK, Aldredge H, Hershberg R, Fisher CM. Oculomotor palsy in diabetes mellitus: a clinico-pathological study. Brain. 1970. 93:555–566.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Oculomotor Nerve Palsy due to Ruptured Multiple Anterior Choroidal Artery Aneurysms
- Oculomotor Nerve Palsy in Internal Carotid-Posterior Communicating Artery Aneurysm
- Unilateral Abducens Nerve Palsy Associated with Ruptured Anterior Communicating Artery Aneurysm
- Pituitary Apoplexy Presenting as Isolated Oculomotor Nerve Palsy
- Analysis of Oculomotor Nerve Palsy due to Internal Carotid-Posterior Communicating Artery Aneurysm
