Isolated Left Ventricular Apical Hypoplasia with Infundibular Pulmonary and Aortic Stenosis: a Rare Combination
- Affiliations
-
- 1Department of Radiology, Medical Research Institute, Pusan National University Hospital, Busan 602-739, Korea. jw@pusan.ac.kr
- 2Department of Internal Medicine, Medical Research Institute, Pusan National University Hospital, Busan 602-739, Korea.
- KMID: 1711452
- DOI: http://doi.org/10.3348/kjr.2013.14.6.874
Abstract
- Isolated left ventricular (LV) apical hypoplasia is a rare congenital cardiac anomaly which is not accompanied by other cardiac abnormalities, with the exception of two cases. We report a case of a 33-year-old male patient with isolated LV apical hypoplasia combined with infundibular pulmonary stenosis and aortic stenosis. We review a literature focusing on the characteristic magnetic resonance features and combined cardiac abnormalities.
Keyword
MeSH Terms
Figure
-
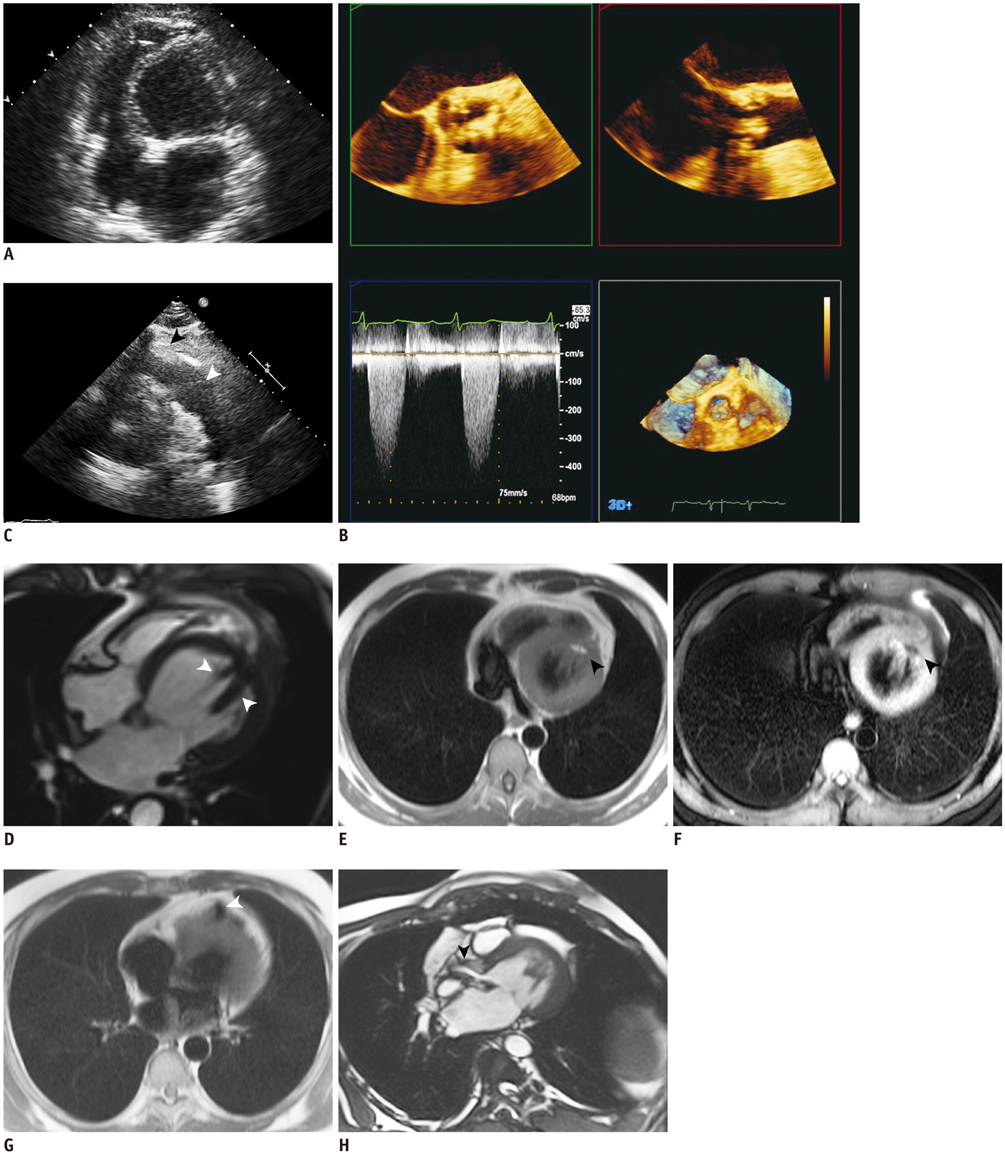
Fig. 1 Thirty-three-old male was diagnosed with isolated LV apical hypoplasia combined with infundibular pulmonary stenosis and aortic stenosis. Echocardiographic images of patient (A-C). A. Apical four-chamber view demonstrates spherically truncated LV with elongated RV wrapped around deficient LV apex. B. Three-dimensional midesophageal transesophageal echocardiographic images of aortic stenosis. Parasternal shortaxis and three-chamber views show aortic calcification with moderate to severe stenosis. At rest, mean pressure gradient was 44 mm Hg and peak velocity was 4.2 m/sec. Calculated aortic orifice is 1.1 cm2. C. Parasternal short-axis view taken during diastole, showing pulmonary valve (white arrowhead), demonstrates thickened muscular infundibulum (black arrowhead). LV = left ventricle, RV = right ventricle. Cardiac MR findings of patient (D-H). D. Four-chamber cardiac MR image taken during diastole shows truncated, spherical LV with rightward bulging of interventricular septum and elongation of RV. Papillary muscles originate from flattened anterior apex (arrowheads). E. Transverse HASTE dark-blood MR image outlines fat within myocardium at LV apex (arrowhead). F. Transverse HASTE dark-blood MR image with fat saturation shows loss of high-signal intensity of deficient LV apex consistent with fatty infiltration, which is characteristic of dysplasia affecting this area (arrowhead). G. Transverse HASTE dark-blood MR image taken during end-systole shows infundibular pulmonary stenosis (arrowhead). H. Static image from three-chamber cardiac MRI examination performed with true fast imaging with steady-state precession shows systolic jet flow, suggestive of aortic stenosis (arrowhead). LV = left ventricle, RV = right ventricle, HASTE = half-fourrer-acquisition single-short turbo spin-echo
Reference
-
1. Fernandez-Valls M, Srichai MB, Stillman AE, White RD. Isolated left ventricular apical hypoplasia: a new congenital anomaly described with cardiac tomography. Heart. 2004; 90:552–555.2. Haffajee JA, Finley JJ, Brooks EL, Kuvin JT, Patel AR. Echocardiographic characterization of left ventricular apical hypoplasia accompanied by a patent ductus arteriosus. Eur J Echocardiogr. 2011; 12:E17.3. Chaowu Y, Xin S, Shihua Z, Jianrong L, Hao W. Complete transposition of the atrioventricular valves associated with left ventricular apical hypoplasia. Circulation. 2011; 124:e538–e539.4. Meléndez G, Muñoz L, Meave A. Isolated left ventricular apical hypoplasia. Rev Esp Cardiol. 2010; 63:984.5. Freedom RM, Black MD, Benson LN. Hypoplastic left heart syndrome. In : Allen HD, Gutgesell HP, Clark EB, Driscoll DJ, editors. Moss and Adams' heart disease in infants, children, and adolescents, including the fetus and young adult. Philadelphia: Lippincott Williams & Wilkins;2001. p. 1011–1026.6. Irving CA, Chaudhari MP. Fatal presentation of congenital isolated left ventricular apical hypoplasia. Eur J Cardiothorac Surg. 2009; 35:368–369.7. Vanhecke TE, Decker J, Leonowicz N, Chinnaiyan KM. Isolated left ventricular apical hypoplasia. Congenit Heart Dis. 2011; 6:646–649.8. Starmer G, Younger JF, Stewart P. Multimodality imaging of isolated left ventricular apical hypoplasia. Eur Heart J. 2012; 33:675.9. Patrianakos AP, Protonotarios N, Zacharaki A, Tsatsopoulou A, Parthenakis FI, Vardas PE. Isolated left ventricular apical hypoplasia: a newly recognized unclassified cardiomyopathy. J Am Soc Echocardiogr. 2010; 23:1336.e1–1336.e4.10. Tumabiene KD, Magpali AE Jr, Chiong L, Jara RD, Abarquez RF Jr, Abelardo NS. A plump and fatty heart: isolated left ventricular apical hypoplasia. Echocardiography. 2012; 29:E193–E196.11. Ong CC, Hia CP, Lim TC, Teo LL. Isolated left-ventricular apical hypoplasia presenting as a left-ventricular mass on echocardiography. Pediatr Cardiol. 2012; 33:1456–1457.12. Motwani M, Witte KK, Plein S, Greenwood JP. Isolated left ventricular apical hypoplasia evaluated by cardiovascular magnetic resonance and gadolinium enhancement techniques. J Am Coll Cardiol. 2011; 58:2355.13. Marin C, Sanchez ML, Maroto E, Ossaba S, Ruiz Y, Zabala JI. MR imaging of isolated left ventricular apical hypoplasia. Pediatr Radiol. 2007; 37:703–705.14. Flett AS, Elliott PM, Moon JC. Images in cardiovascular medicine. Cardiovascular magnetic resonance of isolated left ventricular apical hypoplasia. Circulation. 2008; 117:e504–e505.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Interrupted Aortic Arch with Apical Muscular Ventricular Septal Defect Associating Esophageal Atresia with Tracheoesophageal Fistula
- A Case of Pulmonary Infundibular Stenosis Developed in Ventricular Septal Defect
- Three-Dimensional Endo-Cardiovascular Volume-Rendered Cine Computed Tomography of Isolated Left Ventricular Apical Hypoplasia: A Case Report and Literature Review
- Isolated Right Ventricular Apical Hypoplasia: A Case Report with 18 Years of Follow Up
- A Case of Right Ventricular Infundibular and Pulmonic Valve Infective Endocarditis
