Initial Experience with the New Double-lumen Scepter Balloon Catheter for Treatment of Wide-necked Aneurysms
- Affiliations
-
- 1Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul 110-746, Korea.
- 2Department of Radiology, Yonsei University College of Medicine, Severance Hospital, Seoul 120-752, Korea. bmoon21@hanmail.net
- 3Department of Radiology, Yonsei University College of Medicine, Gangnam Severance Hospital, Seoul 135-720, Korea.
- KMID: 1711443
- DOI: http://doi.org/10.3348/kjr.2013.14.5.832
Abstract
OBJECTIVE
A new double-lumen balloon catheter was being developed for the treatment of cerebral aneurysms. The purpose of this study is to report our initial experience of a double-lumen balloon catheter for the treatment of wide-necked aneurysms.
MATERIALS AND METHODS
Seventeen patients (mean age, 63 years; range, 45-80 years) with wide-necked, with or without a branch-incorporated aneurysms, (10 ruptured and 9 unruptured) were treated with balloon-assisted coil embolization using a double-lumen balloon catheter (Scepter C(TM) or Scepter XC(TM)) for 7 months after being introduced to our country. Locations of the aneurysms were posterior communicating artery (n = 7), anterior communicating artery or A2 (n = 7), middle cerebral artery (MCA) bifurcation (n = 3), basilar artery tip (n = 1) and anterior choroidal artery (n = 1). The initial clinical and angiographic outcomes were retrospectively evaluated.
RESULTS
Coil embolization was successfully completed in all 19 aneurysms, resulting in complete occlusions (n = 18) or residual neck (n = 1). In one procedure, a thrombus formation was detected at the neck portion of the ruptured MCA bifurcation aneurysm near to the end of the procedure. It was completely resolved with an intra-arterial infusion of Glycoprotein IIb/IIIa inhibitor (Tirofiban, 1.0 mg) without any clinical sequela. There were no treatment-related events in the remaining 18 aneurysms. At discharge, functional neurological state improved in 11 patients (10 patients with ruptured aneurysm and 1 with unruptured aneurysm presenting with mass symptoms) and 6 patients with unruptured aneurysms had no newly developed symptoms.
CONCLUSION
In this preliminary case series, the newly developed double-lumen Scepter balloon appears to be a safe and convenient device for coil embolization of wide-necked aneurysms.
Keyword
MeSH Terms
Figure
-
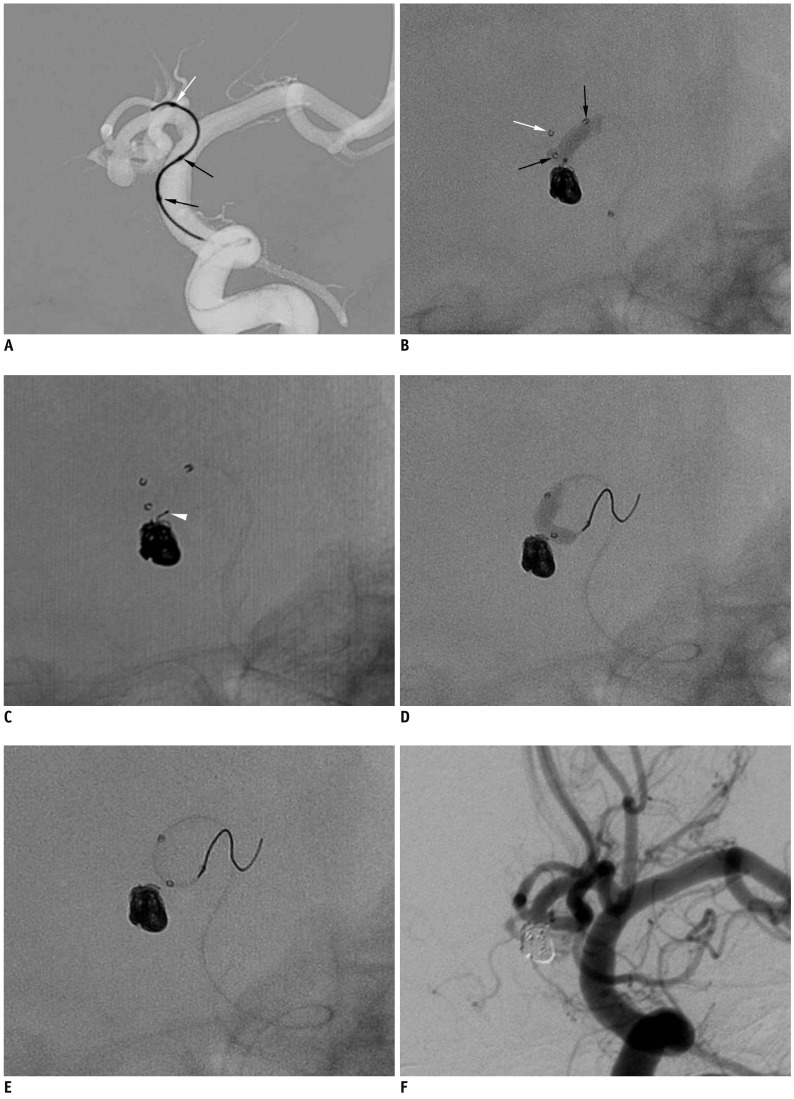
Fig. 1 Case 1. 72-year-old man with ruptured anterior communicating artery aneurysm.A. Advancement of Scepter balloon catheter over 0.014-inch microguidewire that was prepositioned at anterior cerebral artery A1 portion. B. Scepter balloon-assisted coil embolization performed after removal of microguidewire. C. Coil tail (white arrowhead) protruded after balloon deflation. D, E. Scepter balloon catheter is repositioned from right A2 to left A2 using microguidewire and is used to push coil tail in sac. F. Final control angiogram shows complete occlusion of aneurysm sac without any coil loop protrusion. Note that white arrow indicates distal tip marker of Scepter balloon catheter and black arrows indicate proximal and distal markers of balloon itself.
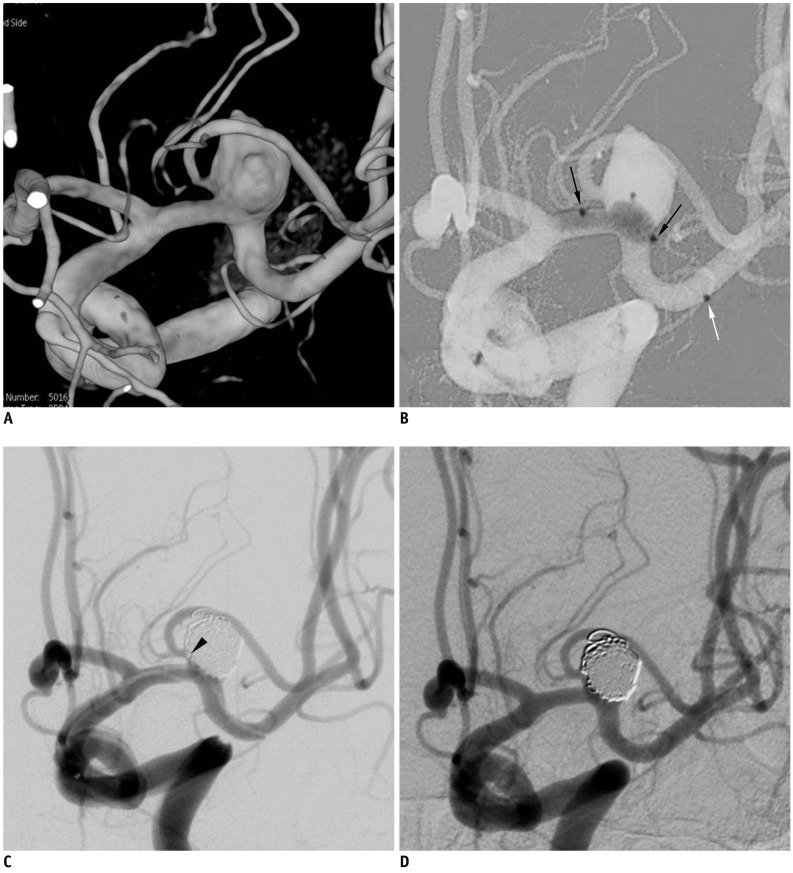
Fig. 2 Case 2. 66-year-old woman with ruptured aneurysm at middle left cerebral artery.A. Three-dimension reconstruction angiogram reveals large aneurysm at middle left cerebral artery bifurcation. Note that superior branch is incorporated into sac. B. After placement of balloon across aneurysm neck, gradual over-inflation causes substantial portion of balloon to herniate into aneurysm sac. C. At end of procedure, small thrombus (black arrowhead) is detected at aneurysm neck, close to origin of superior branch. D. After intraarterial infusion of Glycoprotein inhibitor, 30-minutes follow-up angiogram shows resolution of thrombus and complete occlusion of aneurysm sac. Note that white arrow indicates distal tip marker of Scepter balloon catheter and black arrows indicate proximal and distal markers of balloon itself.
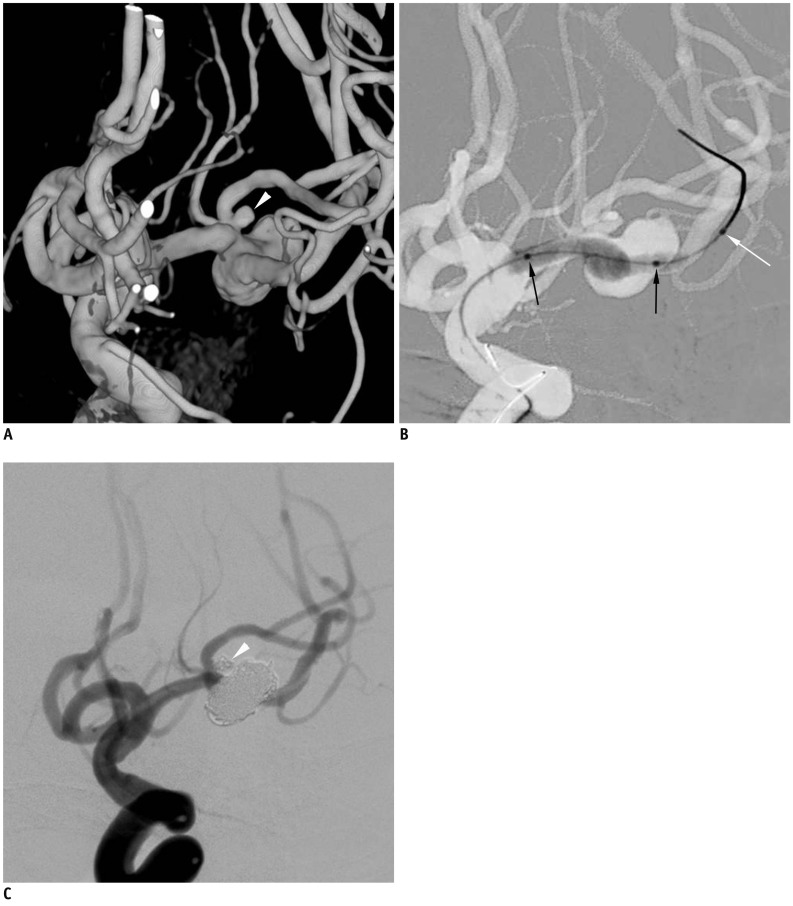
Fig. 3 Case 3. 80-year-old woman with ruptured middle left cerebral artery aneurysms.A. Three-dimensional reconstruction angiogram reveals large aneurysm at middle left cerebral artery bifurcation and another very small aneurysm (white arrowhead) close to aneurysm neck at superior branch. B. After positioning Scepter balloon catheter across aneurysm neck, gradual over-inflation leads to herniation of central portion of balloon into large aneurysm sac. C. After balloon-assisted coil embolization of both aneurysms, final control angiogram shows complete occlusion of both aneurysms and well-preserved superior and inferior divisions. Black arrows indicate proximal and distal balloon markers of Scepter balloon catheter. White arrow indicated distal tip marker of Scepter balloon catheter (black arrows, proximal and distal balloon markers; white arrow, tip marker of balloon catheter).
Cited by 2 articles
-
A Newly-Developed Flow Diverter (FloWise) for Internal Carotid Artery Aneurysm: Results of a Pilot Clinical Study
Byung Moon Kim, Keun Young Park, Jae Whan Lee, Joonho Chung, Dong Joon Kim, Dong Ik Kim
Korean J Radiol. 2019;20(3):505-512. doi: 10.3348/kjr.2018.0421.Comparison Between Balloon-Assisted and Stent-Assisted Technique for Treatment of Unruptured Internal Carotid Artery Aneurysms
Keun Young Park, Byung Moon Kim, Dong Joon Kim
Neurointervention. 2016;11(2):99-104. doi: 10.5469/neuroint.2016.11.2.99.
Reference
-
1. Kim BM, Park SI, Kim DJ, Kim DI, Suh SH, Kwon TH, et al. Endovascular coil embolization of aneurysms with a branch incorporated into the sac. AJNR Am J Neuroradiol. 2010; 31:145–151. PMID: 19749218.
Article2. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; 34:1398–1403. PMID: 12775880.
Article3. Jeon P, Kim BM, Kim DI, Park SI, Kim KH, Kim DJ, et al. Reconstructive endovascular treatment of fusiform or ultrawide-neck circumferential aneurysms with multiple overlapping enterprise stents and coiling. AJNR Am J Neuroradiol. 2012; 33:965–971. PMID: 22268079.
Article4. Kim BM, Kim DJ, Kim DI. Stent application for the treatment of cerebral aneurysms. Neurointervention. 2011; 6:53–70. PMID: 22125751.
Article5. Roh HG, Chun YI, Choi JW, Cho J, Moon WJ, Solander S. Retrograde stent placement for coil embolization of a wide-necked posterior inferior cerebellar artery aneurysm. Korean J Radiol. 2012; 13:510–514. PMID: 22778576.
Article6. Kim DJ, Suh SH, Kim BM, Kim DI, Huh SK, Lee JW. Hemorrhagic complications related to the stent-remodeled coil embolization of intracranial aneurysms. Neurosurgery. 2010; 67:73–78. discussion 78-79. PMID: 20559093.
Article7. Piotin M, Blanc R, Spelle L, Mounayer C, Piantino R, Schmidt PJ, et al. Stent-assisted coiling of intracranial aneurysms: clinical and angiographic results in 216 consecutive aneurysms. Stroke. 2010; 41:110–115. PMID: 19959540.8. Shapiro M, Becske T, Sahlein D, Babb J, Nelson PK. Stent-supported aneurysm coiling: a literature survey of treatment and follow-up. AJNR Am J Neuroradiol. 2012; 33:159–163. PMID: 22033717.
Article9. Sluzewski M, van Rooij WJ, Beute GN, Nijssen PC. Balloon-assisted coil embolization of intracranial aneurysms: incidence, complications, and angiography results. J Neurosurg. 2006; 105:396–399. PMID: 16961133.
Article10. Pierot L, Cognard C, Anxionnat R, Ricolfi F. CLARITY Investigators. Remodeling technique for endovascular treatment of ruptured intracranial aneurysms had a higher rate of adequate postoperative occlusion than did conventional coil embolization with comparable safety. Radiology. 2011; 258:546–553. PMID: 21131582.
Article11. Pierot L, Cognard C, Spelle L, Moret J. Safety and efficacy of balloon remodeling technique during endovascular treatment of intracranial aneurysms: critical review of the literature. AJNR Am J Neuroradiol. 2012; 33:12–15. PMID: 21349960.
Article12. Gory B, Kessler I, Seizem Nakiri G, Riva R, Al-Khawaldeh M, Mounayer C. Initial experience of intracranial aneurysm embolization using the balloon remodeling technique with Scepter C, a new double-lumen balloon. Interv Neuroradiol. 2012; 18:284–287. PMID: 22958766.
Article13. Spiotta AM, Miranpuri A, Hawk H, Chaudry MI, Turk AS, Turner RD. Balloon remodeling for aneurysm coil embolization with the coaxial lumen Scepter C balloon catheter: initial experience at a high volume center. J Neurointerv Surg. 2012; [Epub ahead of print].
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of "Double-catheter" Technique in GDC Treatment of Intracranial Wide-necked Aneurysm
- Balloon-Assisted Coil Embolization and Balloon Angioplasty for Post Subarachnoid Hemorrhage Vasospasm: Initial Experience with Scepter Mini Balloon
- Double-Balloon-Assisted Coiling for Wide-Necked Posterior Communicating Artery Aneurysms with a Fetal-Type Variant of the Posterior Cerebral Artery: A Case Series
- Initial experience with Scepter Mini dual lumen balloon for embolization of cerebrovascular diseases
- Endovascular Treatment of Wide-Necked Intracranial Aneurysms Using Balloon-Assisted Technique with HyperForm Balloon
