MRI Features of Spinal Epidural Angiolipomas
- Affiliations
-
- 1Department of Radiology, The First Affiliated Hospital of Soochow University, Jiangsu 215006, China. hch5305@163.com
- 2Department of Radiology, Wuxi People's Hospital Affiliated to Nanjing Medical University, Jiangsu 214023, China.
- 3Department of Radiology, The Second Affiliated Hospital of Nantong University, Jiangsu 226001, China.
- KMID: 1711439
- DOI: http://doi.org/10.3348/kjr.2013.14.5.810
Abstract
OBJECTIVE
To describe the MRI findings in ten patients of spinal epidural angiolipoma for differentiated diagnosis presurgery.
MATERIALS AND METHODS
Ten surgically proved cases of spinal epidural angiolipomas were retrospectively reviewed, and the lesion was classified according to the MR findings.
RESULTS
Ten tumors were located in the superior (n = 4), middle (n = 2), or inferior (n = 4) thoracic level. The mass, with the spindle shape, was located in the posterior epidural space and extended parallel to the long axis of the spine. All lesions contained a fat and vascular element. The vascular content, correlating with the presence of hypointense regions on T1-weighted imaging (T1WI) and hyperintense signals on T2-weighted imaging, had marked enhancement. However, there were no flow void signs on MR images. All tumors were divided into two types based on the MR features. In type 1 (n = 3), the mass was predominantly composed of lipomatous tissue (> 50%) and contained only a few small angiomatous regions, which had a trabeculated or mottled appear. In type 2 (n = 7), the mass, however, was predominantly composed of vascular components (> 50%), which presented as large foci in the center of the mass.
CONCLUSION
Most spinal epidural angiolipomas exhibit hyperintensity on T1WI while the hypointense region on the noncontrast T1WI indicates to be vascular, which manifests an obvious enhancement with gadolinium administration.
MeSH Terms
Figure
-

Fig. 1 Type 1 epidural angiolipoma. 50-year-old female with bilateral lower extremity adynamia of 18 months. A. Noncontrast T1-weighted sagittal MR image showed homogeneous hyperintense mass compressing spinal cord and scarred with thin-strips or spots of vessels (arrow). Mass was spindle-shaped as longitudinal axis parallel to that of spine and both ends were spinous and pen-like. B. Noncontrast T2-weighted sagittal MR image showed that mass was also hyperintense. C. Postcontrast T1-weighted sagittal MR image showed obvious enhancement of mass. D. Postcontrast T1-weighted axial MR image showed mass displacing thecal sac anteriorly.
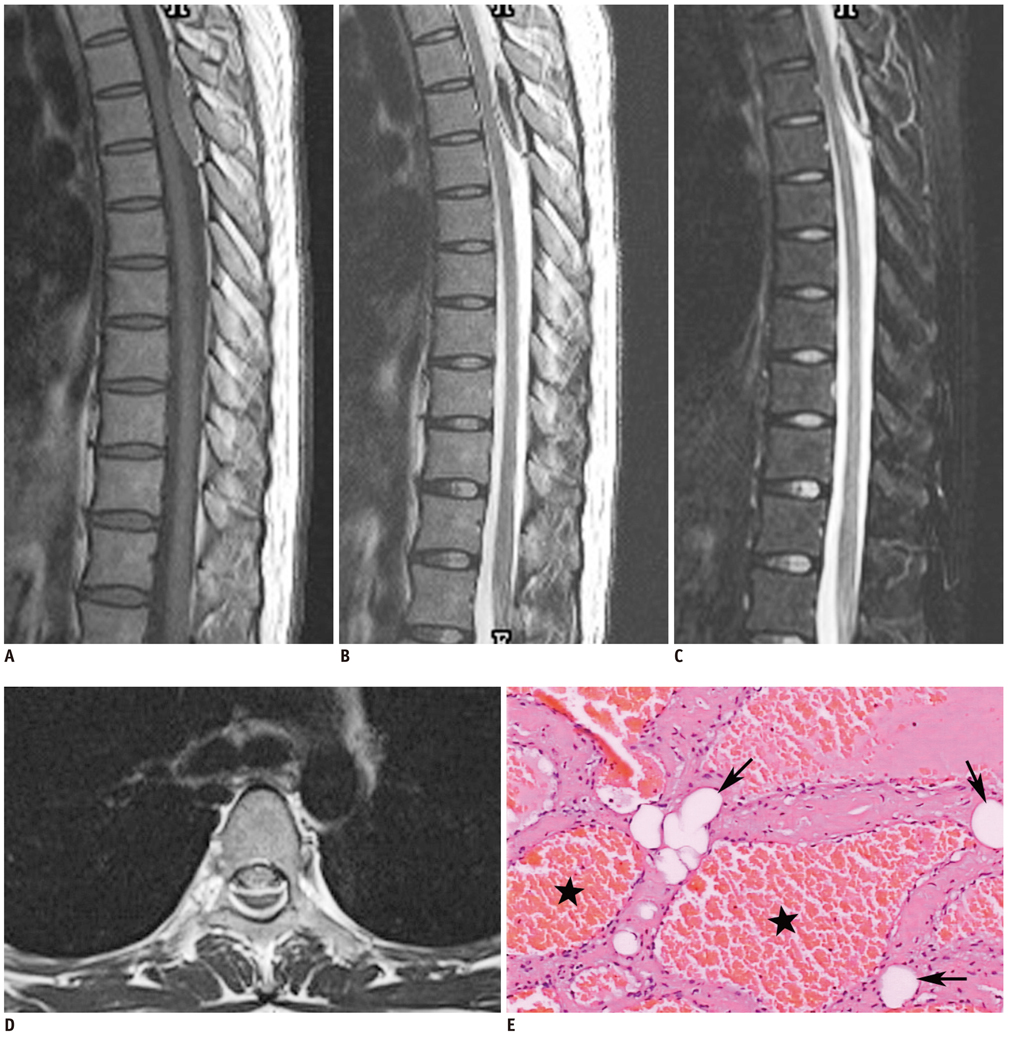
Fig. 2 Epidural angiolipoma with intratumoral hematoma. 24-year-old female with suddenly paraplegia of 6 days. A. Noncontrast T1-weighted sagittal MR image showed epidural isointense mass with little hyperintense surrounding by. B. Noncontrast T2-weighted sagittal MR image showed that central of mass is hypointense but periphery is hyperintense. C. Fat-saturated T2-weighted sagittal MR image showed no decrease of hyperintense region. D. Noncontrast T1-weighted axial MR image showed mass slightly displacing thecal sac anteriorly. E. Microscopically, tumor was composed of abundant vascular channels (★) and mature adipose tissue (arrow), indicative of angiolipoma (haematoxylin and eosin stained, original magnification × 200).
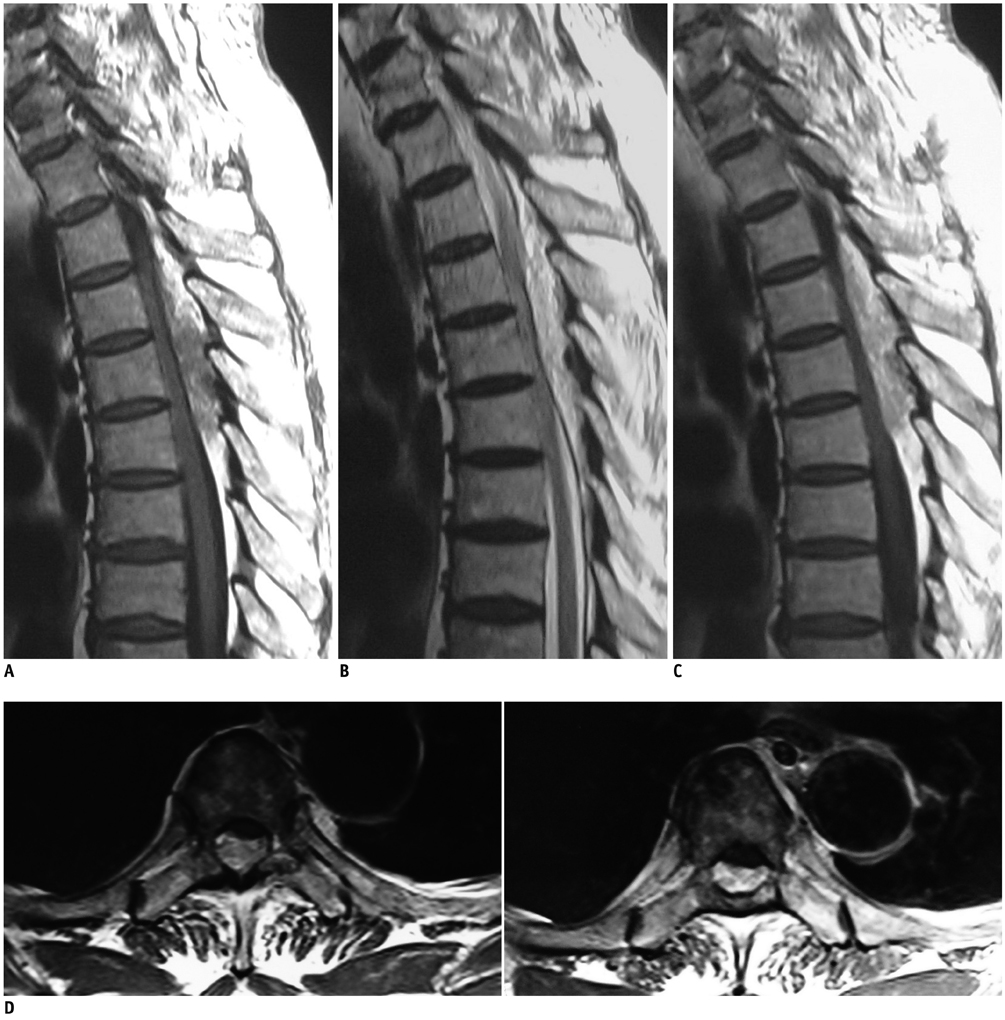
Fig. 3 Type 2 epidural angiolipoma. 77-year-old male with bilateral lower extremity numbness of 4 months. A. Noncontrast T1-weighted sagittal MR image showed inhomogeneous mass that had component which demonstrated as being hypointense, while portions of tumor which were hyperintense were seen above and below hypointense area. B. Noncontrast T2-weighted sagittal MR image showed that mass which compressed spinal cord was hyperintense. Slit-like low signal could be seen between tumor and spinal. C. Postcontrast T1-weighted sagittal MR image showed inhomogeneous enhancement of mass without any sign of blood flow-void phenomenon. D. Postcontrast T1-weighted axial MR image showed mass locating in posterior epidural space of spinal.
Cited by 1 articles
-
Spinal Angiolipomas : Clinical Characteristics, Surgical Strategies and Prognosis
Xiaolei Zhang, Sheng Dong, Guoqin Wang, Huifang Zhang, James Jin Wang, Guihuai Wang
J Korean Neurosurg Soc. 2022;65(1):49-56. doi: 10.3340/jkns.2021.0005.
Reference
-
1. Preul MC, Leblanc R, Tampieri D, Robitaille Y, Pokrupa R. Spinal angiolipomas. Report of three cases. J Neurosurg. 1993; 78:280–286.2. Samdani AF, Garonzik IM, Jallo G, Eberhart CG, Zahos P. Spinal angiolipoma: case report and review of the literature. Acta Neurochir (Wien). 2004; 146:299–302. discussion 302.3. Nanassis K, Tsitsopoulos P, Marinopoulos D, Mintelis A, Tsitsopoulos P. Lumbar spinal epidural angiolipoma. J Clin Neurosci. 2008; 15:460–463.4. Ghanta RK, Koti K, Dandamudi S. Spinal epidural angiolipoma: a rare cause of spinal cord compression. J Neurosci Rural Pract. 2012; 3:341–343.5. Berenbruch K. Ein Fall von multiple Angio-lipomen kombiniert mit einem Angiom des Ruckenmarks. Tibingen: 1890.6. Fourney DR, Tong KA, Macaulay RJ, Griebel RW. Spinal angiolipoma. Can J Neurol Sci. 2001; 28:82–88.7. Haddad FS, Abla A, Allam CK. Extradural spinal angiolipoma. Surg Neurol. 1986; 26:473–486.8. Walsh JW, Markesbery WR. Histological features of congenital lipomas of the lower spinal canal. J Neurosurg. 1980; 52:564–569.9. Thomas JE, Miller RH. Lipomatous tumors of the spinal canal. A study of their clinical range. Mayo Clin Proc. 1973; 48:393–340.10. Shibata Y, Sugimoto K, Matsuki T, Nose T. Thoracic epidural angiolipoma--case report. Neurol Med Chir (Tokyo). 1993; 33:316–319.11. Petrella G, Tamburrini G, Lauriola L, Di Rocco C. Spinal epidural angiolipoma complicated by an intratumoral abscess. Case report. J Neurosurg. 2005; 103:2 Suppl. 166–169.12. Shuangshoti S, Hongsaprabhas C. Intraspinal epidural angiolipoma. J Med Assoc Thai. 1979; 62:457–460.13. Poon TP, Behbahani M, Matoso IM, Katz MA, Pearl M. Epidural angiolipoma with spinal cord compression. J Natl Med Assoc. 1988; 80:347–349.14. Hungs M, Paré LS. Spinal angiolipoma: case report and literature review. J Spinal Cord Med. 2008; 31:315–318.15. Provenzale JM, McLendon RE. Spinal angiolipomas: MR features. AJNR Am J Neuroradiol. 1996; 17:713–719.16. Gelabert-González M, García-Allut A. Spinal extradural angiolipoma: report of two cases and review of the literature. Eur Spine J. 2009; 18:324–335.17. Sakaida H, Waga S, Kojima T, Kubo Y, Matsubara T, Yamamoto J. Thoracic spinal angiomyolipoma with extracanal extension to the thoracic cavity. A case report. Spine (Phila Pa 1976). 1998; 23:391–394.18. Turgut M. Spinal angiolipomas: report of a case and review of the cases published since the discovery of the tumour in 1890. Br J Neurosurg. 1999; 13:30–40.19. Leu NH, Chen CY, Shy CG, Lu CY, Wu CS, Chen DC, et al. MR imaging of an infiltrating spinal epidural angiolipoma. AJNR Am J Neuroradiol. 2003; 24:1008–1011.20. Akhaddar A, Albouzidi A, Elmostarchid B, Gazzaz M, Boucetta M. Sudden onset of paraplegia caused by hemorrhagic spinal epidural angiolipoma. A case report. Eur Spine J. 2008; 17:Suppl 2. S296–S298.21. Weill A, del Carpio-O'Donovan R, Tampieri D, Melanson D, Ethier R. Spinal angiolipomas: CT and MR aspects. J Comput Assist Tomogr. 1991; 15:83–85.22. Kujas M, Lopes M, Lalam TF, Fohanno D, Poirier J. Infiltrating extradural spinal angiolipoma. Clin Neuropathol. 1999; 18:93–98.23. Zhong W, Huang S, Chen H, Sun H, Cai B, Liu Y, et al. Pure spinal epidural cavernous hemangioma. Acta Neurochir (Wien). 2012; 154:739–745.
