Irreversible Electroporation of a Hepatocellular Carcinoma Lesion Adjacent to a Transjugular Intrahepatic Portosystemic Shunt Stent Graft
- Affiliations
-
- 1Department of Radiology, University Medical Center Regensburg, Regensburg D-93053, Germany. christoph.niessen@ukr.de
- 2Department of Anaesthesia, University Medical Center Regensburg, Regensburg D-93053, Germany.
- KMID: 1711436
- DOI: http://doi.org/10.3348/kjr.2013.14.5.797
Abstract
- We report in a 65-year-old man hepatocellular carcinoma adjacent to a transjugular intrahepatic portosystemic shunt stent-graft which was successfully treated with irreversible electroporation (IRE). IRE is a new non-thermal tissue ablation technique which uses electrical pulses to induce cell necrosis by irreversible membrane poration. IRE proved to be more advantageous in the ablation of perivascular tumor with little injury to the surrounding structures.
Keyword
MeSH Terms
Figure
-
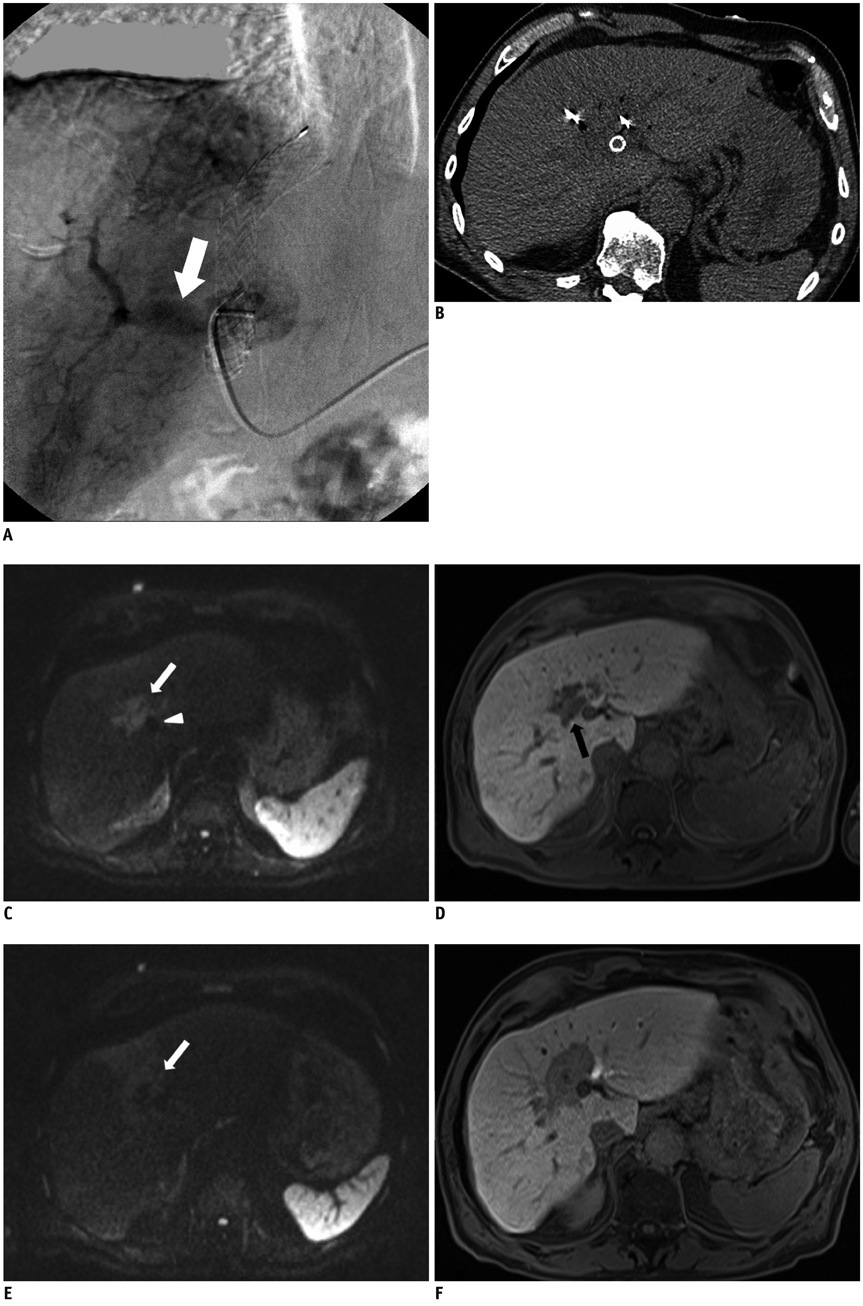
Fig. 1 Pre-interventional angiography and intra-procedural CT scan and pre- and post-ablation MR images. A. Angiographic image during TACE. Celiac arteriography shows diffuse arteriovenous shunts (white arrow). TACE failed due to shunt. B. CT image during CT fluoroscopy-guided IRE. Precontrast CT shows low-attenuation ablation defect abutting TIPS stent graft (arrows). Note deployment of electrodes adjacent to TIPS stent graft. TACE = transarterial chemoembolization, TIPS = transjugular intrahepatic portosystemic shunt. C-F. Pre- and post-ablation MR images. C. Preablation diffusion-weighted MR Image (b = 1000 sec/mm2) shows slightly hyperintense HCC (white arrow) adjacent to TIPS stent graft (white arrowhead). D. Preablation T1-weighted image during hepatobiliary phase shows hypointense HCC which measures 2.2 × 4.0 cm (black arrow). E. 8-week postablation diffusion-weighted MR-image (b = 1000 sec/mm2) shows complete ablation of HCC (arrow). F. 8-week postablation T1-weighted MR-image shows hypointense sharp demarcation of ablation zone. HCC = hepatocellular carcinoma, TIPS = transjugular intrahepatic portosystemic shunt
Cited by 1 articles
-
Comparison of Chronologic Change in the Size and Contrast-Enhancement of Ablation Zones on CT Images after Irreversible Electroporation and Radiofrequency Ablation
Jonas Scheck, Philipp Bruners, David Schindler, Christiane Kuhl, Peter Isfort
Korean J Radiol. 2018;19(4):560-567. doi: 10.3348/kjr.2018.19.4.560.
Reference
-
1. Yun BL, Lee JM, Baek JH, Kim SH, Lee JY, Han JK, et al. Radiofrequency ablation for treating liver metastases from a non-colorectal origin. Korean J Radiol. 2011; 12:579–587.2. Patterson EJ, Scudamore CH, Owen DA, Nagy AG, Buczkowski AK. Radiofrequency ablation of porcine liver in vivo: effects of blood flow and treatment time on lesion size. Ann Surg. 1998; 227:559–565.3. Dupuy DE, Aswad B, Ng T. Irreversible electroporation in a Swine lung model. Cardiovasc Intervent Radiol. 2011; 34:391–395.4. Lee EW, Loh CT, Kee ST. Imaging guided percutaneous irreversible electroporation: ultrasound and immunohistological correlation. Technol Cancer Res Treat. 2007; 6:287–294.5. Deodhar A, Dickfeld T, Single GW, Hamilton WC Jr, Thornton RH, Sofocleous CT, et al. Irreversible electroporation near the heart: ventricular arrhythmias can be prevented with ECG synchronization. AJR Am J Roentgenol. 2011; 196:W330–W335.6. Kingham TP, Karkar AM, D'Angelica MI, Allen PJ, Dematteo RP, Getrajdman GI, et al. Ablation of perivascular hepatic malignant tumors with irreversible electroporation. J Am Coll Surg. 2012; 215:379–387.7. Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208–1236.8. Cho YK, Kim JK, Kim MY, Rhim H, Han JK. Systematic review of randomized trials for hepatocellular carcinoma treated with percutaneous ablation therapies. Hepatology. 2009; 49:453–459.9. Kamusella P, Wiggermann P, Wissgott C, Andresen R, Stroszczynski C. [Thermal protection of targeted air instillation in CT-guided radiofrequency ablation]. Rofo. 2011; 183:952–955.10. Raman SS, Lu DS, Vodopich DJ, Sayre J, Lassman C. Minimizing diaphragmatic injury during radio-frequency ablation: efficacy of subphrenic peritoneal saline injection in a porcine model. Radiology. 2002; 222:819–823.11. Lencioni R, Crocetti L. Local-regional treatment of hepatocellular carcinoma. Radiology. 2012; 262:43–58.12. Chang NK, Shin SS, Kim JW, Kim HJ, Jeong YY, Heo SH, et al. Effect of ultrasound-guided radiofrequency ablation in incompletely treated hepatocellular carcinoma after transcatheter arterial chemoembolization. Korean J Radiol. 2012; 13:Suppl 1. S104–S111.13. Lee J, Lee JM, Yoon JH, Lee JY, Kim SH, Lee JE, et al. Percutaneous radiofrequency ablation with multiple electrodes for medium-sized hepatocellular carcinomas. Korean J Radiol. 2012; 13:34–43.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- RE: Irreversible Electroporation of a Hepatocellular Carcinoma Lesion Adjacent to a Transjugular Intrahepatic Portosystemic Shunt Stent Graft
- Percutaneous retrieval of a misplaced transjugular intrahepatic portosystemic shunt stent using the rigid endobronchial forceps
- A new and improved transjugular intrahepatic portosystemic shunt (TIPS) stent graft: Controlled expansion
- Recanalization of an Occluded Intrahepatic Portosystemic Covered Stent via the Percutaneous Transhepatic Approach
- Complete Remission of Refractory Hepatic Hydrothorax in Patient with Advanced Liver Cirrhosis and Hepatocellular Carcinoma Using Transjugular Intrahepatic Portosystemic Shunt
