A Case of Tuberculous Liver Abscess Developed during Chemotherapy for Tuberculous Peritonitis as Paradoxical Response
- Affiliations
-
- 1Department of Internal Medicine, Medical Research Institute, Pusan National University School of Medicine and Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea. luckyace@han
- KMID: 1711282
- DOI: http://doi.org/10.4166/kjg.2013.62.1.64
Abstract
- Tuberculous liver abscesses are rare. Paradoxical response in tuberculosis is common and occurred between 2 weeks and 12 weeks after anti-tuberculous medication. We report here a case of tuberculous liver abscess that developed in a paradoxical response during chemotherapy for tuberculous peritonitis in a 23-year-old male. He was hospitalized, complaining of ascites, epigastric pain. He was diagnosed tuberculous peritonitis by expiratory laparoscopic biopsy and took medication for tuberculosis. After 2 months, a hepatic lesion was detected with CT scan incidentally. Chronic granulomatous inflammation was seen in ultrasound-guided liver biopsy, and tuberculous liver abscess was diasnosed. It was considered as paradoxical response, rather than treatment failure or other else because clinical symptoms of peritoneal tuberculosis and CT scan improved. After continuing initial anti-tuberculous medication, he was successfully treated. Herein, we report a case of tuberculous liver abscess as paradoxical response while treating peritoneal tuberculosis without changing anti-tuberculous treatment regimen.
MeSH Terms
-
Antitubercular Agents/*adverse effects/*therapeutic use
DNA, Bacterial/analysis
Humans
Laparoscopy
Liver/pathology/ultrasonography
Liver Abscess/*chemically induced/*diagnosis/microbiology
Male
Mycobacterium tuberculosis/genetics/isolation & purification
Necrosis/pathology
Peritoneum/pathology
Peritonitis, Tuberculous/*drug therapy
Tomography, X-Ray Computed
Tuberculosis/*diagnosis/microbiology
Young Adult
Antitubercular Agents
DNA, Bacterial
Figure
-
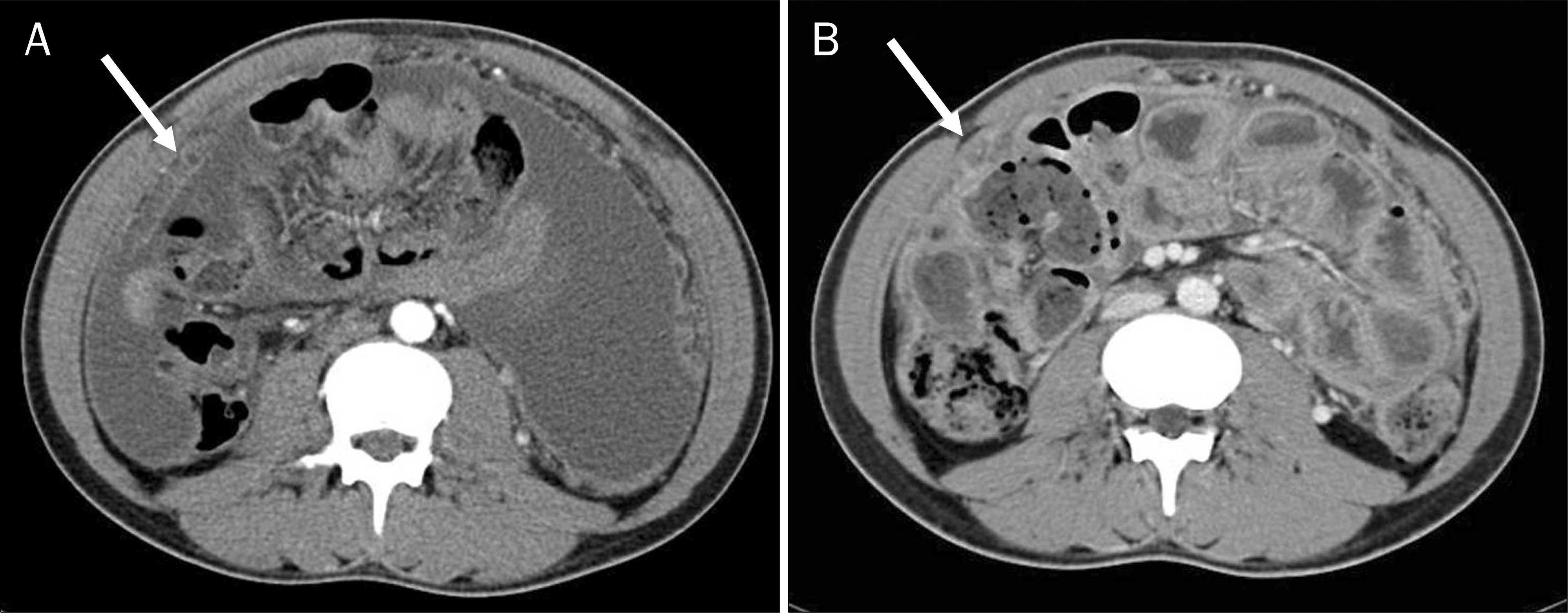
Fig. 1. (A) Initial pelvic CT before antituberculosis therapy showed a lot of ascites and omental smudge (arrow). (B) Follow-up CT 2 months after starting antituberculosis therapy showed decrease of ascites and omental smudge (arrow).

Fig. 2. Gross findings through the laparoscope. Diffuse whitish nodules with ascites were noted on the peritoneum.

Fig. 3. Microscopic findings of the peritoneum. Multinucleated giant cell and chronic granulomatous inflammation with caseous necrosis was noted (H&E, ×200).

Fig. 4. (A) After treatment for 2 months, a new small low-attenuation nodule was noted on subcapsular area of the S5 segment (arrow). (B) After treatment for 6 months, the size of lesion increased (arrow). (C) After treatment for 13 months, the lesion disappeared (arrow).

Fig. 5. Microscopic findings of the liver. The specimen showed chronic granulomatous inflammation with caseous necrosis (H&E, ×100).
Cited by 1 articles
-
단독 간농양으로 발현된 속립성 결핵
Chang Won Ha, Sang Deok Shin, Myung Ji Goh, Byeong Geun Song, Wonseok Kang, Dong Hyun Sinn, Geum-Youn Gwak, Yong-Han Paik, Moon Seok Choi, Joon Hyeok Lee
Korean J Gastroenterol. 2025;85(1):78-82. doi: 10.4166/kjg.2024.119.
Reference
-
References
1. Hersch C. Tuberculosis of the liver. A study of 200 cases. S Afr Med J. 1964; 38:857–863.2. Rab SM, Beg MZ. Tuberculous liver abscess. Br J Clin Pract. 1977; 31:157–158.3. Hung SC, Chang SC. New pulmonary lesions during therapy for extrapulmonary tuberculosis. Chest. 1999; 116:1794–1797.
Article4. Onal IK, Bayraktar Y, Unal S. Paradoxical deterioration during the course of antituberculous treatment. J Natl Med Assoc. 2006; 98:954–955.5. Al-Majed SA. Study of paradoxical response to chemotherapy in tuberculous pleural effusion. Respir Med. 1996; 90:211–214.
Article6. Cheng VC, Ho PL, Lee RA, et al. Clinical spectrum of paradoxical deterioration during antituberculosis therapy in non-HIV-infected patients. Eur J Clin Microbiol Infect Dis. 2002; 21:803–809.
Article7. Kim SH, Chung HY, Lee GD, et al. Clinical characteristics of paradoxical response to chemotherapy in pulmonary tuberculosis. Tuberc Respir Dis. 2002; 53:27–35.
Article8. Blumberg HM, Burman WJ, Chaisson RE, et al. American Thoracic Society, Centers for Disease Control and Prevention and the Infectious Diseases Society. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003; 167:603–662.9. Kok KY, Yapp SK. Isolated hepatic tuberculosis: report of five cases and review of the literature. J Hepatobiliary Pancreat Surg. 1999; 6:195–198.
Article10. Tan TC, Cheung AY, Wan WY, Chen TC. Tuberculoma of the liver presenting as a hyperechoic mass on ultrasound. Br J Radiol. 1997; 70:1293–1295.
Article11. Kim YR. The CT findings and clinical course of intraperitoneal tuberculous abscess. Korean J Med. 2008; 74:233–234.12. Orlovic D, Smego RA Jr. Paradoxical tuberculous reactions in HIV-infected patients. Int J Tuberc Lung Dis. 2001; 5:370–375.13. Jung SW, Kim JB, Choi JS, et al. Development of a tuberculous liver abscess as a paradoxical response. Korean J Med. 2012; 83:87–92.
Article14. Jung MK, Lee HJ, Kim MJ, et al. Paradoxical response to chemotherapy in tuberculous pleural effusion. Pediatr Allergy Respir Dis. 2009; 19:71–77.15. Versalovic J. Manual of clinical microbiology. 10th ed.Washington: ASM Press;2011.16. Yano S, Kobayashi K, Kato K, Tokuda Y, Ikeda T, Takeyama H. Paradoxical worsening of pulmonary Mycobacterium abscessus. Respir Med. 2007; 101:868–870.
Article17. Jang KJ, Jwa CS, Kim KH, Kang JK. Paradoxical deterioration of intramedullary spinal tuberculomas during antituberculous therapy. J Korean Neurosurg Soc. 2007; 41:408–410.18. Kim SY, Oh TH, Seo JY, et al. A case of tuberculous peritonitis developed during chemotherapy for tuberculous pleurisy as paradoxical response. Korean J Gastroenterol. 2011; 57:379–383.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Development of a Tuberculous Liver Abscess as a Paradoxical Response
- The CT findings and clinical course of intraperitoneal tuberculous abscess
- A Case of Tuberculous Peritonitis Developed during Chemotherapy for Tuberculous Pleurisy as Paradoxical Response
- Tuberculous Iliopsoas Muscle Abscess Associated with Multiple Intraabdominal and Thoracic Abscesses in 9-year-old Boy
- A Case Report of Tuberculous Brain Abscess and Tuberculous Peritonitis Developing Due to Paradoxical Reactions
