Cementless Total Hip Arthroplasty for Patients with Crowe Type III or IV Developmental Dysplasia of the Hip: Two-Stage Total Hip Arthroplasty Following Skeletal Traction after Soft Tissue Release for Irreducible Hips
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul National University Boramae Hospital, Seoul, Korea. ksyoon@brm.co.kr
- 2Department of Orthopedic Surgery, Seoul National University Hospital, Seoul, Korea.
- KMID: 1705541
- DOI: http://doi.org/10.4055/cios.2013.5.3.167
Abstract
- BACKGROUND
Total hip arthroplasty (THA) for severe developmental dysplasia of the hip (DDH) is a technically demanding procedure for arthroplasty surgeons, and it is often difficult to reduce the hip joint without soft tissue release due to severe flexion contracture. We performed two-stage THAs in irreducible hips with expected lengthening of the affected limb after THA of over 2.5 cm or with flexion contractures of greater than 30 degrees in order to place the acetabular cup in the true acetabulum and to prevent neurologic deficits associated with acute elongation of the limb. The purpose of this study is to evaluate the outcomes of cementless THA in patients with severe DDH with a special focus on the results of two-stage THA.
METHODS
Retrospective clinical and radiological evaluations were done on 17 patients with Crowe type III or IV developmental DDH treated by THA. There were 14 women and 3 men with a mean age of 52.3 years. Follow-ups averaged 52 months. Six cases were treated with two-stage THA followed by surgical hip liberalization and skeletal traction for 2 weeks.
RESULTS
The mean Harris hip score improved from 40.9 to 89.1, and mean leg length discrepancy (LLD) in 13 unilateral cases was reduced from 2.95 to 0.8 cm. In the patients who underwent two-stage surgery, no nerve palsy was observed, and the single one-stage patient with incomplete peroneal nerve palsy recovered fully 4 weeks postoperatively.
CONCLUSIONS
The short-term clinical and radiographic outcomes of primary cementless THA for patients with Crowe type III or IV DDH were encouraging. Two-stage THA followed by skeletal traction after soft tissue release could provide alternative solutions to the minimization of limb shortenings or LLD without neurologic deficits in highly selected patients.
MeSH Terms
-
Adult
Aged
Arthroplasty, Replacement, Hip/*instrumentation/*methods
Female
Femur/radiography/surgery
Hip/radiography/surgery
Hip Dislocation, Congenital/pathology/radiography/*surgery
Hip Joint/pathology/radiography/surgery
Hip Prosthesis
Humans
Ilium/radiography/surgery
Male
Middle Aged
Orthopedic Fixation Devices
Retrospective Studies
Traction
Figure
-
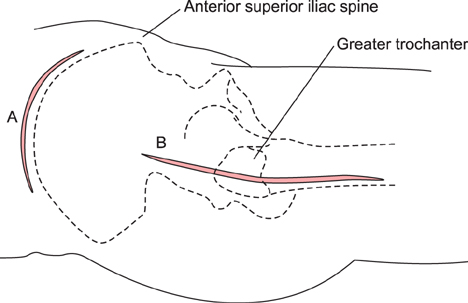
Fig. 1 A curvilinear incision over the iliac crest was used to elevate abductor muscles off the ilium subperiosteally (A). The hip was exposed through a modified Hardinge's approach (B).
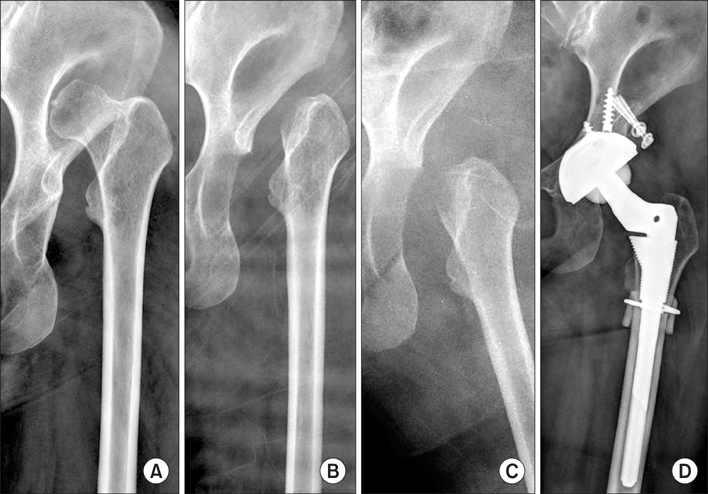
Fig. 2 Preoperative plain radiograph showing Crowe type IV developmental dysplasia of the hip (A). During the first stage, surgical hip liberalization with abductor slide and skeletal traction for 2 weeks were performed (B, C). During the second stage, a total hip arthroplasty and subtrochanteric shortening osteotomy were performed due to difficult reduction (D).
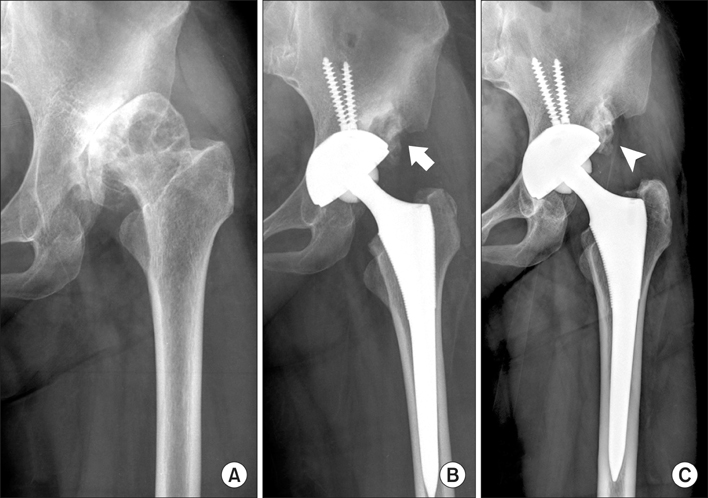
Fig. 3 Preoperative radiograph showing Crowe type III developmental dysplasia of the hip (A). One-stage total hip arthroplasty was performed and the superolateral aspect of the acetabulum was augmented with an autogenous femoral head bone graft (arrow, B). Solid union was confirmed by plain radiography at 3 years after surgery (arrowhead, C).
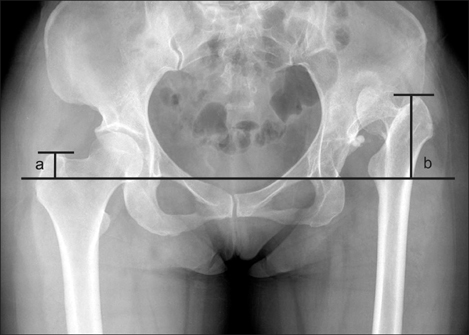
Fig. 4 In cases of unilateral developmental dysplasia of the hip, leg length discrepancy was defined as the difference between the distances from the interteardrop line and the greater trochanter tip in the affected and contralateral hips on anteroposterior hip radiographs and was measured before and after surgery (b - a).
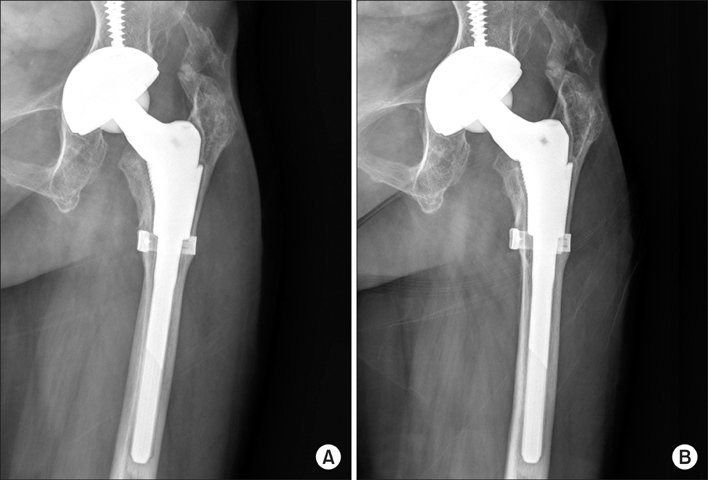
Fig. 5 Postoperative plain radiograph taken at 2 years after surgery showing a diffuse radiolucent line of less than 2 mm in Gruen zones 1 and 7 (A). This was considered to indicate stable fibrous fixation because no change was observed 1 year later (B).
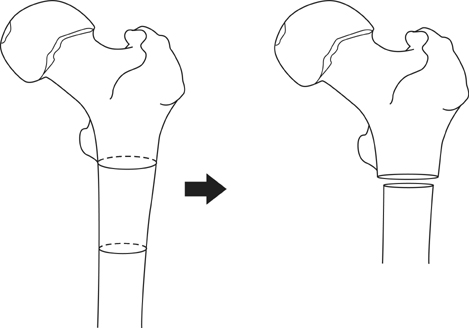
Fig. 6 Incongruence between canal diameters of apposed fragments after subtrochanteric shortening is exacerbated by excessive resection of the diaphyseal segment.
Cited by 1 articles
-
The Result of Revision Total Hip Arthroplasty in Patients with Metallosis Following a Catastrophic Failure of a Polyethylene Liner
Hong Suk Kwak, Jeong Joon Yoo, Young-Kyun Lee, Kyung-Hoi Koo, Kang Sup Yoon, Hee Joong Kim
Clin Orthop Surg. 2015;7(1):46-53. doi: 10.4055/cios.2015.7.1.46.
Reference
-
1. Argenson JN, Flecher X, Parratte S, Aubaniac JM. Anatomy of the dysplastic hip and consequences for total hip arthroplasty. Clin Orthop Relat Res. 2007; 465:40–45.
Article2. Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am. 1979; 61(1):15–23.
Article3. Anwar MM, Sugano N, Masuhara K, Kadowaki T, Takaoka K, Ono K. Total hip arthroplasty in the neglected congenital dislocation of the hip: a five- to 14-year follow-up study. Clin Orthop Relat Res. 1993; (295):127–134.4. Cameron HU, Botsford DJ, Park YS. Influence of the Crowe rating on the outcome of total hip arthroplasty in congenital hip dysplasia. J Arthroplasty. 1996; 11(5):582–587.
Article5. Charnley J, Feagin JA. Low-friction arthroplasty in congenital subluxation of the hip. Clin Orthop Relat Res. 1973; (91):98–113.
Article6. Eskelinen A, Helenius I, Remes V, Ylinen P, Tallroth K, Paavilainen T. Cementless total hip arthroplasty in patients with high congenital hip dislocation. J Bone Joint Surg Am. 2006; 88(1):80–91.
Article7. Takao M, Ohzono K, Nishii T, Miki H, Nakamura N, Sugano N. Cementless modular total hip arthroplasty with subtrochanteric shortening osteotomy for hips with developmental dysplasia. J Bone Joint Surg Am. 2011; 93(6):548–555.
Article8. Togrul E, Ozkan C, Kalaci A, Gulsen M. A new technique of subtrochanteric shortening in total hip replacement for Crowe type 3 to 4 dysplasia of the hip. J Arthroplasty. 2010; 25(3):465–470.
Article9. Biant LC, Bruce WJ, Assini JB, Walker PM, Walsh WR. Primary total hip arthroplasty in severe developmental dysplasia of the hip: ten-year results using a cementless modular stem. J Arthroplasty. 2009; 24(1):27–32.
Article10. Reikeras O, Haaland JE, Lereim P. Femoral shortening in total hip arthroplasty for high developmental dysplasia of the hip. Clin Orthop Relat Res. 2010; 468(7):1949–1955.
Article11. Nagoya S, Kaya M, Sasaki M, Tateda K, Kosukegawa I, Yamashita T. Cementless total hip replacement with subtrochanteric femoral shortening for severe developmental dysplasia of the hip. J Bone Joint Surg Br. 2009; 91(9):1142–1147.
Article12. Krych AJ, Howard JL, Trousdale RT, Cabanela ME, Berry DJ. Total hip arthroplasty with shortening subtrochanteric osteotomy in Crowe type-IV developmental dysplasia. J Bone Joint Surg Am. 2009; 91(9):2213–2221.
Article13. Makita H, Inaba Y, Hirakawa K, Saito T. Results on total hip arthroplasties with femoral shortening for Crowe's group IV dislocated hips. J Arthroplasty. 2007; 22(1):32–38.
Article14. Masonis JL, Patel JV, Miu A, et al. Subtrochanteric shortening and derotational osteotomy in primary total hip arthroplasty for patients with severe hip dysplasia: 5-year follow-up. J Arthroplasty. 2003; 18:3 Suppl 1. 68–73.
Article15. Park MS, Kim KH, Jeong WC. Transverse subtrochanteric shortening osteotomy in primary total hip arthroplasty for patients with severe hip developmental dysplasia. J Arthroplasty. 2007; 22(7):1031–1036.
Article16. DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976; (121):20–32.
Article17. Engh CA, Bobyn JD, Glassman AH. Porous-coated hip replacement: the factors governing bone ingrowth, stress shielding, and clinical results. J Bone Joint Surg Br. 1987; 69(1):45–55.
Article18. Linde F, Jensen J, Pilgaard S. Charnley arthroplasty in osteoarthritis secondary to congenital dislocation or subluxation of the hip. Clin Orthop Relat Res. 1988; 227:164–171.
Article19. Pagnano W, Hanssen AD, Lewallen DG, Shaughnessy WJ. The effect of superior placement of the acetabular component on the rate of loosening after total hip arthroplasty. J Bone Joint Surg Am. 1996; 78(7):1004–1014.20. Paavilainen T. Total hip replacement for developmental dysplasia of the hip. Acta Orthop Scand. 1997; 68(1):77–84.21. Edwards BN, Tullos HS, Noble PC. Contributory factors and etiology of sciatic nerve palsy in total hip arthroplasty. Clin Orthop Relat Res. 1987; (218):136–141.
Article22. Jasty M, Webster W, Harris W. Management of limb length inequality during total hip replacement. Clin Orthop Relat Res. 1996; (333):165–171.
Article23. Harley JM, Wilkinson JA. Hip replacement for adults with unreduced congenital dislocation: a new surgical technique. J Bone Joint Surg Br. 1987; 69(5):752–755.
Article24. Chin KR, Brick GW. Reattachment of the migrated ununited greater trochanter after revision hip arthroplasty: the abductor slide technique. A review of four cases. J Bone Joint Surg Am. 2000; 82(3):401–408.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cementless Total Hip Replacement Arthroplasty with Subtrochanteric Shortening Osteotomy in Crowe IV Developmental Dysplasia of the Hip
- Cementless Total Hip Arthroplasty in Dysplastic Hips
- Total Hip Replacement in Unreduced Hip Dislocation
- Revision for Loosened Total Hip Replacement Arthroplasty
- Implant Design in Cementless Hip Arthroplasty
