Candida Septic Arthritis with Rice Body Formation: A Case Report and Review of Literature
- Affiliations
-
- 1Department of Radiology, Gachon University, Gil Hospital, Incheon 405-760, Korea. youme34@gilhospital.com
- 2Department of Pathology, Gachon University, Gil Hospital, Incheon 405-760, Korea.
- 3Department of Orthopedic Surgery, Gachon University, Gil Hospital, Incheon 405-760, Korea.
- KMID: 1705461
- DOI: http://doi.org/10.3348/kjr.2013.14.3.465
Abstract
- Rice body formation in a joint or bursa is a rare condition, and is usually associated with rheumatoid arthritis or tuberculous arthritis. Here we describe a case of multiple rice body formation in a shoulder joint and in adjacent bursae, which was confirmed to be due to septic arthritis by Candida species. To the best of our knowledge, rice body formation in Candida septic arthritis in an immune-competent patient has not been previously reported.
Keyword
MeSH Terms
Figure
-
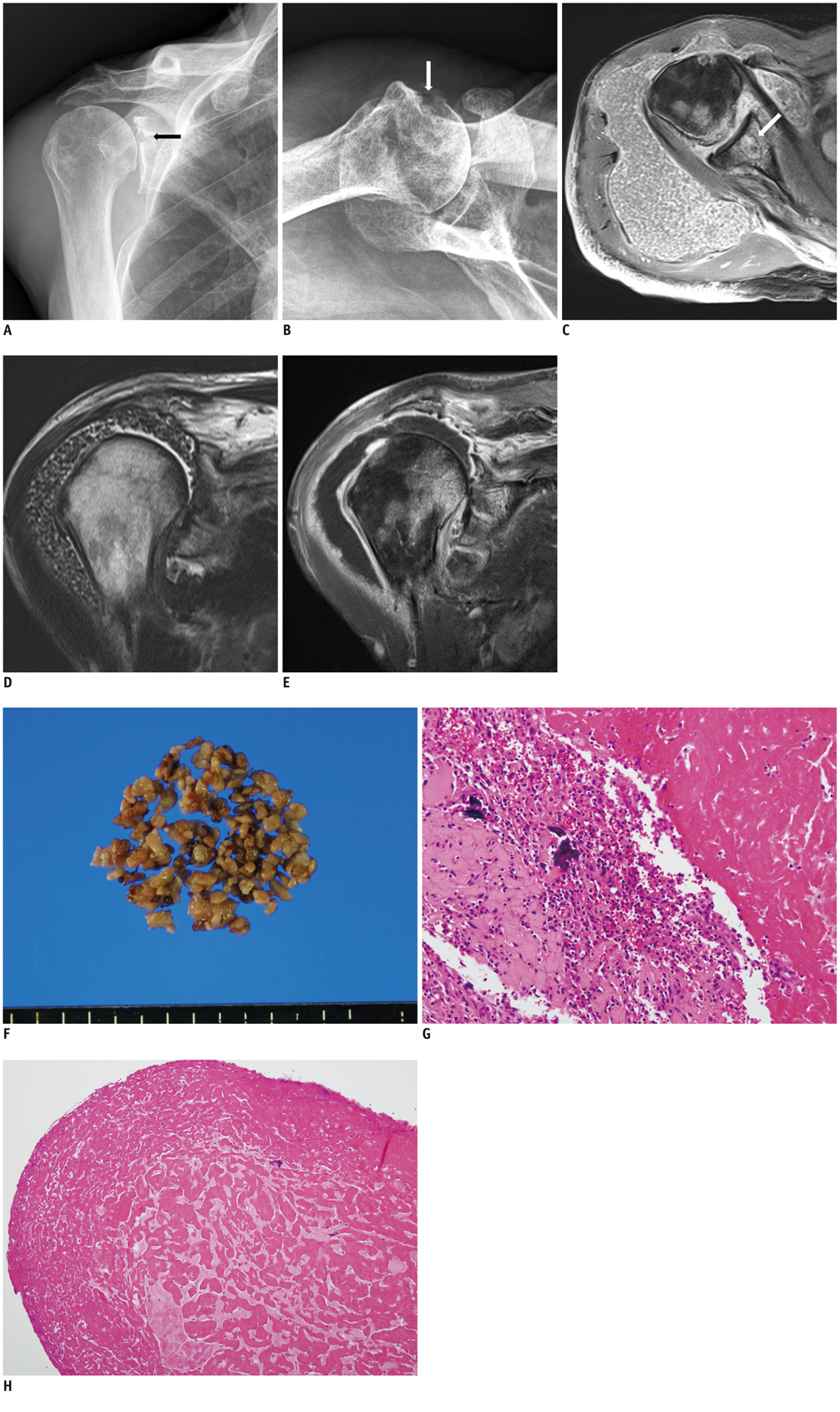
Fig. 1 Imaging and pathologic findings of Candida septic arthritis in right shoulder in a 74-year-old man. A, B. Anteroposterior (A) and axillary (B) radiographs of right shoulder show small bone erosions at glenoid (black arrow) and humeral head (white arrow). Superior migration of humeral head indicates rotator cuff tear. C-E. Axial fat-suppressed proton-density weighted image (C) and coronal T2-weighted image (D) show innumerable rice bodies in right shoulder joint, subacromial-subdeltoid bursa, and subcoracoid bursa. Coronal fat-suppressed T1-weighted image after gadolinium enhancement (E) shows diffuse thickened synovium with enhancement suggestive of synovitis. Bone marrow edema in humeral head and glenoid (C-E) with small subchondral bone erosion at glenoid (arrow in C) suggests osseous involvement of inflammation. F. Resected specimen includes multiple rice bodies of few millimeters in size. G. Resected bursa shows infiltration of chronic inflammatory cells with fibrin deposition and dystrophic calcification (H&E, × 200). H. Rice body is mainly composed of fibrin with some inflammatory cells (H&E, × 100).
Reference
-
1. Reise H. Die Reiskorpschen in tuberculs erkranken synovalsacken [in German]. Dtsch Z Chir. 1895. 42:1.2. Hsu CY, Lu HC, Shih TT. Tuberculous infection of the wrist: MRI features. AJR Am J Roentgenol. 2004. 183:623–628.3. Popert AJ, Scott DL, Wainwright AC, Walton KW, Williamson N, Chapman JH. Frequency of occurrence, mode of development, and significance or rice bodies in rheumatoid joints. Ann Rheum Dis. 1982. 41:109–117.4. Amrami KK, Ruggieri AP, Sundaram M. Radiologic case study. Rheumatoid arthritis with rice bodies. Orthopedics. 2004. 27:350426–427.5. Lee EY, Rubin DA, Brown DM. Recurrent Mycobacterium marinum tenosynovitis of the wrist mimicking extraarticular synovial chondromatosis on MR images. Skeletal Radiol. 2004. 33:405–408.6. Thevenon A, Cocheteux P, Duquesnoy B, Mestdagh H, Lecomte-Houcke M, Delcambre B. Subacromial bursitis with rice bodies as a presenting feature of seronegative rheumatoid arthritis. Arthritis Rheum. 1987. 30:715–716.7. Chau CL, Griffith JF, Chan PT, Lui TH, Yu KS, Ngai WK. Rice-body formation in atypical mycobacterial tenosynovitis and bursitis: findings on sonography and MR imaging. AJR Am J Roentgenol. 2003. 180:1455–1459.8. Tyllianakis M, Kasimatis G, Athanaselis S, Melachrinou M. Rice-body formation and tenosynovitis of the wrist: a case report. J Orthop Surg (Hong Kong). 2006. 14:208–211.9. Ergun T, Lakadamyali H, Aydin O. Multiple rice body formation accompanying the chronic nonspecific tenosynovitis of flexor tendons of the wrist. Radiat Med. 2008. 26:545–548.10. Griffith JF, Peh WC, Evans NS, Smallman LA, Wong RW, Thomas AM. Multiple rice body formation in chronic subacromial/subdeltoid bursitis: MR appearances. Clin Radiol. 1996. 51:511–514.11. Iyengar K, Manickavasagar T, Nadkarni J, Mansour P, Loh W. Bilateral recurrent wrist flexor tenosynovitis and rice body formation in a patient with sero-negative rheumatoid arthritis: a case report and review of literature. Int J Surg Case Rep. 2011. 2:208–211.12. Lin KM, Lai JH, Chang CC, Lin CK, Chang DM, Chen CH. Formation of numerous rice bodies: an unusual finding of adult-onset Still's disease. Clin Rheumatol. 2008. 27:Suppl 2. S55–S57.13. Li-Yu J, Clayburne GM, Sieck MS, Walker SE, Athreya BH, DeHoratius RJ, et al. Calcium apatite crystals in synovial fluid rice bodies. Ann Rheum Dis. 2002. 61:387–390.14. Cheung HS, Ryan LM, Kozin F, McCarty DJ. Synovial origins of Rice bodies in joint fluid. Arthritis Rheum. 1980. 23:72–76.15. Trofa D, Gácser A, Nosanchuk JD. Candida parapsilosis, an emerging fungal pathogen. Clin Microbiol Rev. 2008. 21:606–625.16. Chen A, Wong LY, Sheu CY, Chen BF. Distinguishing multiple rice body formation in chronic subacromial-subdeltoid bursitis from synovial chondromatosis. Skeletal Radiol. 2002. 31:119–121.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Candida Parapsilosis Arthritis Involving the Ankle in a Diabetes Patient: A Case Report1
- A Septic Abortion Caused by Candida glabrata Chorioamnionitis Following in Vitro Fertilization and Embryo Transfer
- Multiple Rice Bodies in Subacromial Space: A Case Report
- Surgical Treatment of Multiple Rice Bodies in Chronic Subacromial and Subdeltoid Bursitis: A Case Report
- Candida Arthritis Presenting as a Huge Popliteal Cyst in a Patient with Rheumatoid Arthritis: A Case Report and Review of the Literature
