Surgical Correction and Osteosynthesis for Cranial Displaced Pelvic Nonunion: Technical Note and Two Cases Report Regarding Anterior Correction and Osteosynthesis Following Posterior Release
- Affiliations
-
- 1Department of Orthopedic Surgery, Daejeon St. Mary's Hospital, School of Medicine, The Catholic University of Korea, Daejeon, Korea. weonkim@hotmail.com
- KMID: 1703114
- DOI: http://doi.org/10.12671/jkfs.2014.27.2.151
Abstract
- Nonunion of an unstable pelvic fracture with cranial displacement pelvic surgery is technically difficult due to a large amount of bleeding and the risk of nerve damage. In addition, surgical correction of leg length discrepancy by reduction of a dislocated sacroiliac joint is in high demand. Nevertheless, when a patient is strongly disabled by a pelvic deformity, surgical correction may be necessary. Two patients with pelvic deformity were treated successfully by surgical correction and osteosynthesis.
MeSH Terms
Figure
-
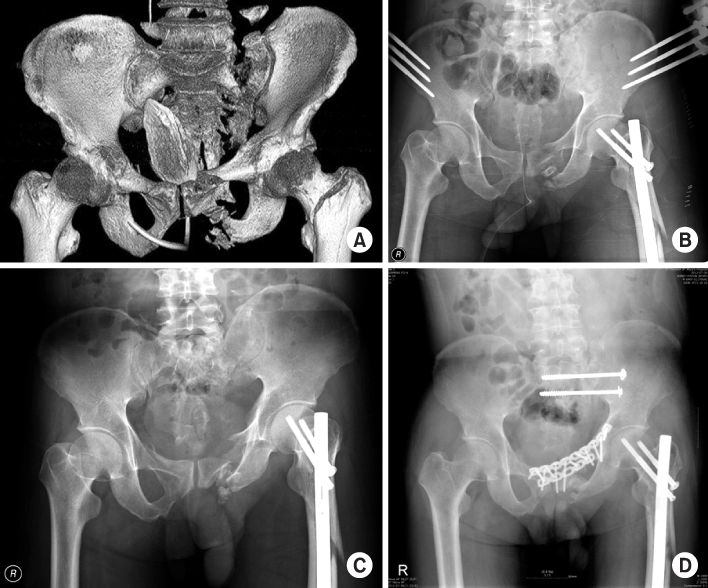
Fig. 1 (A) Initial post-accident computed tomography scan showing both a rami fracture and a left sacral wing fracture (Tile type C). (B) Pelvic reduction and stabilization with anterior pelvic external fixator only. (C) Six months after the accident, simple radiographs showing superior migration of the left hemipelvis and nonunion of the fracture site. (D) Simple radiographs after surgical correction showing decreased cranial displacement.

Fig. 2 (A) Approximately 3 cm cranial displacement of right hemipelvis. (B) One year after surgical correction, simple radiographs showing anatomical reduction and bony union.
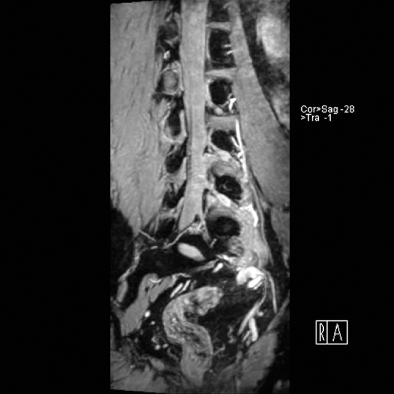
Fig. 3 Preoperative magnetic resonance imaging showing L5 nerve root, tracks inferior over the sacral wing.

Fig. 4 (A) Postoperative computed tomography (CT) scan showing that the S1 sacroiliac screws lie on a safety zone, angled 10 degrees anteriorly. (B) Postoperative CT scan showing that the S2 sacroiliac screws lie on a safety zone, parallel to the floor.
Reference
-
1. Kellam JF, McMurtry RY, Paley D, Tile M. The unstable pelvic fracture. Operative treatment. Orthop Clin North Am. 1987; 18:25–41.2. Tile M. Pelvic ring fractures: should they be fixed? J Bone Joint Surg Br. 1988; 70:1–12.
Article3. van den Bosch EW, van Zwienen CM, van Vugt AB. Fluoroscopic positioning of sacroiliac screws in 88 patients. J Trauma. 2002; 53:44–48.
Article4. Matta JM, Dickson KF, Markovich GD. Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res. 1996; (329):199–206.
Article5. Mears DC, Velyvis J. Surgical reconstruction of late pelvic post-traumatic nonunion and malalignment. J Bone Joint Surg Br. 2003; 85:21–30.
Article6. Rousseau MA, Laude F, Lazennec JY, Saillant G, Catonné Y. Two-stage surgical procedure for treating pelvic malunions. Int Orthop. 2006; 30:338–341.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Testicular Necrosis after Ilioinguinal Approach for Pelvic Nonunion: A Case Report
- Osteosynthesis for Nonunion of the Lateral Condyle of the Humerus
- In Situ Late Metaphyseal Osteosynthesis for the Fractures of the Lateral Humeral Condyle in Children
- The Result of Osteosynthesis of Scaphoid with Matti-Russe Technique and Herbert Screw
- Humeral intramedullary nail bending following trauma: a case report
