1 Case of Bronchial Leiomyoma with Intralobar Pulmonary Sequestration
- Affiliations
-
- 1Department of Internal Medicine, University of Soonchunhyang college of Medicine, Cheonan, Korea. khseo@schch.co.kr
- 2Department of Radiology, University of Soonchunhyang college of Medicine, Cheonan, Korea.
- 3Department of Diagnostic Pathology, University of Soonchunhyang college of Medicine, Cheonan, Korea.
- 4Department of Thoracic Surgery, University of Soonchunhyang college of Medicine, Cheonan, Korea.
- KMID: 1630807
- DOI: http://doi.org/10.4046/trd.2006.60.6.678
Abstract
- Both bronchial leiomyoma and pulmonary sequestration are rare conditions, and to the best of our knowledge there are no reports of the two conditions coexisting. We report a female patient with bronchial leiomyoma with acquired pulmonary sequestration who presented with dyspnea, cough and purulent sputum. The patient had been treated for pneumonia at a local medical clinic. but was transferred to our clinic beacausr there was no clinical improvement. A 3-D computed tomography scan revealed a 1.5 cm sized mass near the distal portion of the left main bronchus and an anomalous artery arising from the aorta. The patient showed clinical improvement after a left lower lobectomy and a ligation of the anomalous artery.
MeSH Terms
Figure
-

Figure 1 Chest PA. (A) Initial film shows consolidation on left lower lobe. (B) Follow up film at 1 day on admission shows total collapse of left lung

Figure 2 Chest CT with CE. (A) Collapse of Left lower lobe due to 1.5 cm sized endobronchial mass (arrow) in distal portion of left main bronchus. (B) Multiple cystic lesion (arrow) at collapse lesion of left lower lobe. (C) Abnormal vessels (arrow) originated from descending aorta at reformed oblique coronal imaging.

Figure 3 Bronchoscopic finding. (A) An impacted mass-like lesion covered a whitish exudate around the distal main bronchus. (B) At 12 days after operation, there was no endobronchial lesion
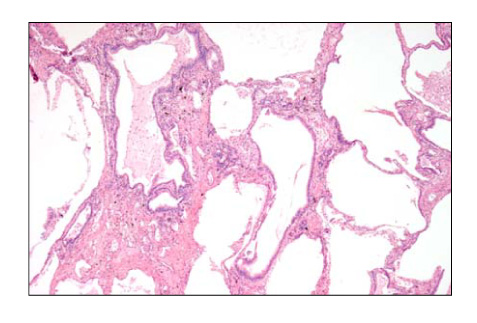
Figure 4 Microscopic finding of pulmonary sequestration. Multicystic spaces lined by cuboidal to columnar epithelium with intervening fibrosis and inflammation (H&E, ×100).
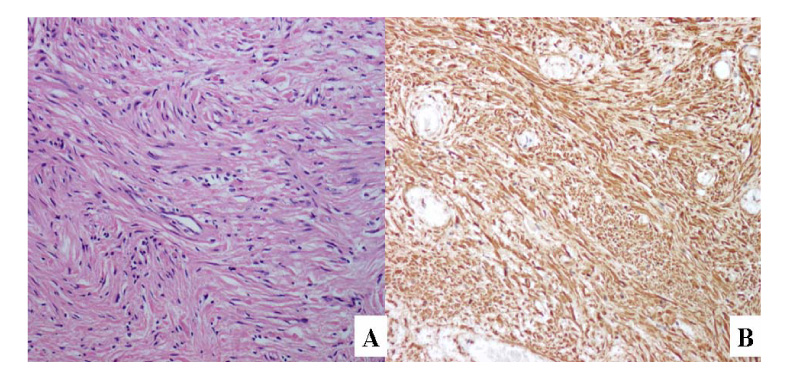
Figure 5 Microscopic findings of leiomyoma. (A) The tumor is formed by interlacing bundles of spindle cells, which has elongated nuclei and eosinophilic fibrillary cytoplasm (H&E, ×200). (B) Immunohistochemically, the tumor shows a diffuse positive reaction for smooth muscle actin (×200).
Reference
-
1. ullen JT, Gaylor DH, Ashburn F. Leiomyoma of the bronchus. Am Rev Respir Dis. 1967. 96:1061–1063.2. wang SC, Pyo CH. A case of pulmonary leiomyoma. J Korean Surg Soc. 1967. 9:493–495.3. Yoo YM, Sohn KH, Kim DS, Ko IH. Leiomyoma of bronchus a case. Korean J Thoracic Cardiovasc Surg. 1985. 18:817–821.4. Lee SC, Park MS, Chung JH, Kim YS, Kim KD, Chang JC, et al. Two case of bronchial leiomyoma initially misdiagnosed as bronchial asthma. Tuberc Respir Dis. 2003. 55:616–622.5. Douzinas M, Sheppard MN, Lennox SC. Leiomyoma of the trachea: an unusual tumour. Thorac Cardiovasc Surg. 1989. 37:285–287.6. White SH, Ibrahim NB, Forrester-Wood CP, Jeyasingham K. Leiomyomas of the lower respiratory tract. Thorax. 1985. 40:306–311.7. Weinbaum PJ, Bors-Koefoed R, Green KW, Prenatt L. Antenatal sonographic findings in a case of intraabdominal pulmonary sequestration. Obstet Gynecol. 1989. 73:860–862.8. Gebauer PW, Mason CB. Intralobar pulmonary sequestration associated with anomalous pulmonary vessels: a nonentity. Dis Chest. 1959. 35:282–288.9. Fraizer AA, Rosado de Christenson ML, Stocker JT, Templetion PA. Intralobar sequestration: radiologicpathologic correlation. Radiographics. 1997. 17:725–745.10. Vera-Roman JM, Sobonya RE, Gomez-Garcia JL, Sanz-Bondia JR, Paris-Romeu F. Leiomyoma of the lung. Cancer. 1983. 52:936–941.11. Yamada H, Katoh O, Yamaguchi T, Natsuaki M, Itoh T. Intrabronchial leiomyoma treated by localized resection via bronchotomy and bronchoplasty. Chest. 1987. 91:283–285.12. Kim HJ, Kang WH, Kang SJ, Chung MP, Choi DC, Kwon OJ, et al. Two cases of bronchial leiomyoma resected by Nd-YAG laser under flexible bronchoscopy. Tuberc Respir Dis. 1996. 43:1028–1034.13. Ayabe H, Tsuji H, Tagawa Y, Tomita M, Tsuda N, Chen J. Endobronchial leiomyoma: report of a case treated by bronchoplasty and a review of the literature. Surg Today. 1995. 25:1057–1060.14. Kilman JW, Battersby JS, Taybi H, Vellios F. Pulmonary sequestration. Arch Surg. 1965. 90:648–657.15. Flye MW, Conley M, Silver D. Spectrum of pulmonary sequestration. Snn Thorscic Surg. 1976. 22:478–482.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endobronchial Leiomyoma Combined with Pulmonary Sequestration: A case report
- Ultrasound and computed tomographic findings of pulmonary sequestration
- Congenital Bronchial Atresia Coexistent with Intralobar Pulmonary Sequestration: A Case Report
- Roentgenogram of the Issue : A Case of Pneumonic Consolidation with Multiple Cavitary Lesion
- Aspergillosis within an Intralobar Sequestration: A Case Report
