A Case of Tuberculous Pleural Effusion Developed after Percutaneous Needle Biopsy of a Solitary Pulmonary Nodule
- Affiliations
-
- 1Departments of Internal Medicine, College of Medicine, Inje University, Busan, Korea. goodoc@gmail.com
- 2Departments of Radiology, College of Medicine, Inje University, Busan, Korea.
- KMID: 1518418
- DOI: http://doi.org/10.4046/trd.2007.63.3.268
Abstract
- A tuberculous pleural effusion may be a sequel to a primary infection or represent the reactivation of pulmonary tuberculosis. It is believed to result from a rupture of a subpleural caseous focus in the lung into the pleural space. It appears that delayed hypersensitivity plays a large role in the pathogenesis of a tuberculous pleural effusion. We encountered a 52 years old man with pleural effusion that developed several days after a CT guided percutaneous needle biopsy of a solitary pulmonary nodule. He was diagnosed with TB pleurisy. It is believed that his pleural effusion probably developed due to exposure of the parenchymal tuberculous focus into the pleural space during the percutaneous needle biopsy. This case might suggest one of the possible pathogeneses of tuberculous pleural effusion.
MeSH Terms
Figure
-
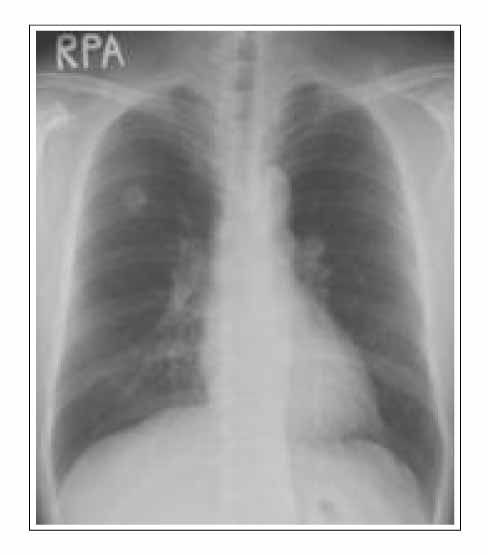
Figure 1 Chest X-ray (initial). Chest x-ray shows a well defined round nodule in right upper lobe.

Figure 2 CT-guided percutaneous biopsy. CT-guided biopsy was done in apical segment of right upper lobe with prone position (A, B).

Figure 3 Chest PA (A) and right decubitus view (B)(2 weeks after biopsy). Chest x-ray shows a lot of pleural fluid shifting in right thorax. Increased patch consolidation around the nodule on RUL.

Figure 4 Chest CT (2 weeks after biopsy). CT showes linear consolidation and pleural effusion along previous biopsy tract (A-D).

Figure 5 Chest PA (4 months later). Chest PA shows disappeared pleural effusion after anti-Tbc medication.
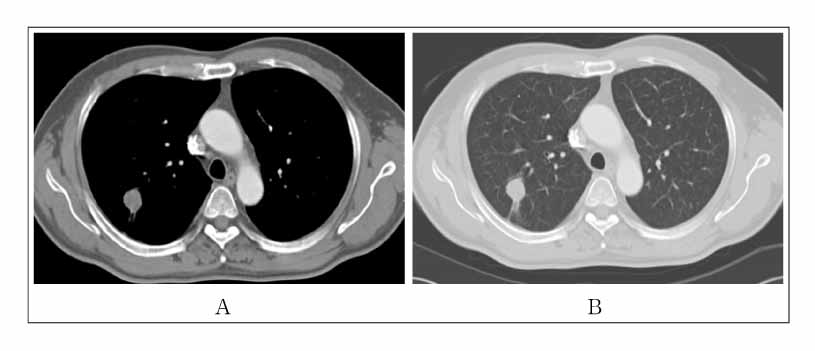
Figure 6 Chest CT (4 months after anti-tbc medication). Chest CT shows no interval change of previous SPN. But pleural effusion and consolidative lesions around the nodule were disappeared (A, B).
Reference
-
1. Berger HW, Mejia E. Tuberculous pleurisy. Chest. 1973. 63:88–92.2. Allen JC, Apicella MA. Experimental pleural effusion as a manifestation of delayed hypersensitivity to tuberculin PPD. J Immunol. 1968. 101:481–487.3. Apicella MA, Allen JC. A physiologic differentiation between delayed and immediate hypersensitivity. J Clin Invest. 1969. 48:250–259.4. Leibowitz S, Kennedy L, Lessof MH. The tuberculin reaction in the pleural cavity and its suppression by antilymphocyte serum. Br J Exp Pathol. 1973. 54:152–162.5. Yamamoto S, Dunn CJ, Willoughby DA. Studies on delayed hypersensitivity pleural exudates in guinea pigs. Demonstration of substances in the cell-free exudate which cause inhibition of mononuclear cell migration in vitro. Immunology. 1976. 30:505–511.6. Antony VB, sahn SA, Antony AC, Repine JE. Bacillus Calmette-Guerin-stimulated neutrophils release chemotaxins for monocytes in rabbit pleural space in vitro. J Clin Invest. 1985. 76:1514–1521.7. Riantawan P, Chaowalit P, Wongsangiem M, Rojanaraweewong P. Diagnostic value of pleural fluid adenosine deaminase in tuberculous pleuritis with reference to HIV coinfection and a bayesian analysis. Chest. 1999. 116:97–103.8. Stead WW, Eichenholz A, Stauss HK. Operative and pathologic findings in twenty-four patients with syndrome of idiopathic pleurisy with effusion, presumably tuberculous. Am Rev Tuberc. 1955. 71:473–502.9. Widstrom O, Nilsson BS. Pleurisy induced by intrapleural BCG in immunized guinea pigs. Eur J Respir Dis. 1982. 63:425–434.10. Fujiwara H, Tsuyuguchi I. Frequency of tuberculin reactive T-lymphocytes in pleural fluid and blood from patients with tuberculous pleurisy. Chest. 1986. 89:530–532.11. Ellner JJ, Barnes PF, Wallis RS, Modlin RL. The immunology of tuberculous pleurisy. Semin Respir Infect. 1988. 3:335–342.12. Cazzadori A, Di Perri G, Marocco S, Carlotto A, Adami T, Concia E. Tuberculous pleurisy after percutaneous needle biopsy of a pulmonary nodule. Respir Med. 1994. 88:477–478.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Percutaneous Pleural Needle Biopsy in the Diagnosis of Lymphocyte Dominant Pleural Effusion
- Thoracoscopic Needle Aspiration Biopsy for a Centrally Located Solitary Pulmonary Nodule
- Video-Assisted Thoracic Surgery Core Needle Biopsy for Pulmonary Nodules in Patients with Impaired Lung Function: Is It Feasible and Safe?
- The Utility of Pleural Adenosine Deaminase for Diagnosis of Differentiating Tuberculous Pleural Effusion in Children
- Diagnostic Thoracoscopy in the Pleural Effusion
