A Case of Cholecysto-gastro-colonic Fistula with Upper Gastrointestinal Bleeding
- Affiliations
-
- 1Department of Gastrointestinal Medicine, Daegu Fatima Hospital, Daegu, Korea. gooddr@hotmail.co.kr
- KMID: 1501653
- DOI: http://doi.org/10.4166/kjg.2013.61.5.290
Abstract
- Biliary enteric fistula is an abnormal pathway often caused by biliary disease. It is difficult to diagnose the disease because patients have nonspecific symptoms. A 67-year-old woman presented with hematemesis and melena. She was diagnosed with Dieulafoy lesion on the gastric antrum and underwent endoscopic hemostasis using hemoclips. Follow-up upper gastrointestinal endoscopy revealed an abnormal opening on a previous treated site that was suggestive of biliary enteric fistula. Abdomen simple X-ray and abdominal dynamic CT scan showed pneumobilia and cholecysto-gastric fistula. The patient had cholecystectomy and wedge resection of the gastric antrum, followed by right extended hemicolectomy because of severe adhesive lesion between the gallbladder and colon. She was diagnosed with cholecysto-gastro-colic fistula postoperatively. We report on this case and give a brief review of the literatures.
Keyword
MeSH Terms
Figure
-

Fig. 1. Upper gastrointestinal endoscopic findings. (A) Fresh blood from an exposed vessel was observed on the great curvature of the gastric antrum. (B) Follow-up examination showed an abnormal opening at the gastric antrum. Yellowish and bubbly contents were drained through the lesion.
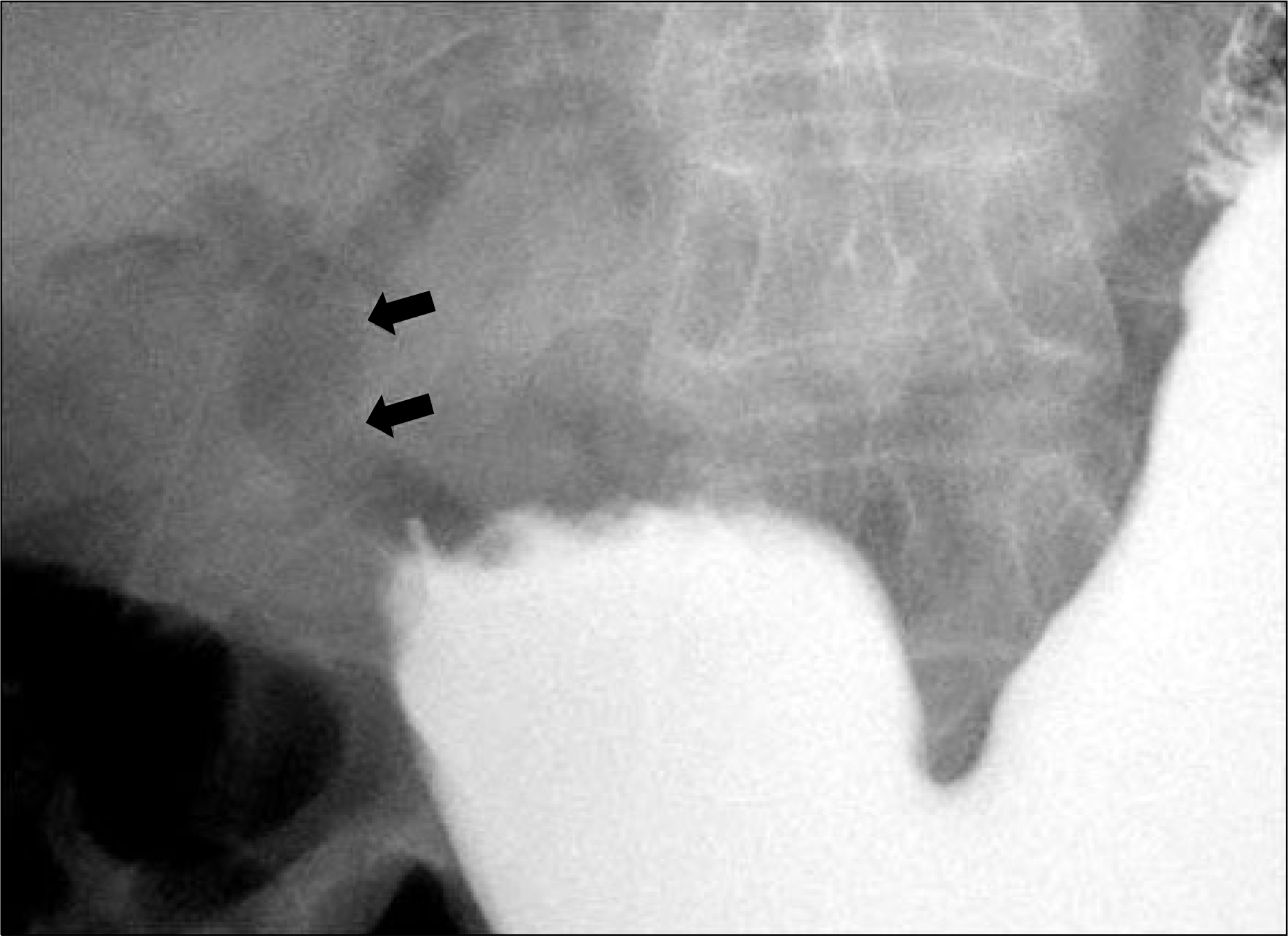
Fig. 2. Abdomen simple X-ray. It revealed pneumobilia (arrows) in the common bile duct, suggesting the presence of biliary enteric fistula.

Fig. 3. Abdominal dynamic CT scan. It showed swelling and fatty infiltration around the gallbladder with contrast enhancement and adhesion of the gallbladder to the gastric antrum (black arrow). Severe inflammatory changes involving the transverse colon were noted (white arrow).

Fig. 4. Histopathologic findings. (A) Macroscopic finding of the surgical specimen showed an orifice of the fistula on the transverse colon. (B) Microscopic finding of the cholecysto-colic fistula showed the formation of necrotic and granulation tissue (H&E, ×20).
Reference
-
References
1. Shim CS, Lee JS, Lee MS, et al. Cholecysto – duodeno – colic fistula: report of one case. Korean J Gastrointest Endosc. 1996; 16:801–806.2. Yamashita H, Chijiiwa K, Ogawa Y, Kuroki S, Tanaka M. The internal biliary fistula–reappraisal of incidence, type, diagnosis and management of 33 consecutive cases. HPB Surg. 1997; 10:143–147.3. Glenn F, Reed C, Grafe WR. Biliary enteric fistula. Surg Gynecol Obstet. 1981; 153:527–531.4. Jang LC, Han SH, Kim SW, Park YH. Biliary-enteric fistula. Korean J Gastroenterol. 1992; 24:827–832.5. Seo JS, Yang SY, Kim JH, et al. A case of choledocho-duode-no-colonic fistula. Korean J Gastrointest Endosc. 2007; 34:278–281.6. Hakim M, Boyd R, Stricoff R, Shaftan G, Saxe A. Cholecystogas-trocolonic fistula with intrahepatic abscess: a rare complication of biliary stone disease. Am Surg. 1997; 63:472–474.7. Elsas LJ, Gilat T. Cholecystocolonic fistula with malabsorption. Ann Intern Med. 1965; 63:481–486.
Article8. LeBlanc KA, Barr LH, Rush BM. Spontaneous biliary enteric fistulas. South Med J. 1983; 76:1249–1252.
Article9. La Greca G, Grasso E, Sofia M, Gagliardo S, Barbagallo F. Complicated duodeno-biliary fistula in bleeding duodenal ulcer: case report an literature review. Ann Ital Chir. 2008; 79:57–61.10. Stempfle B, Diamantopoulos G. Spontaneous cholecysto-ga-stric fistula with massive gastrointestinal bleeding. Endoscopic diagnosis and concrement extraction. Fortschr Med. 1976; 94:444–447.11. Feller ER, Warshaw AL, Schapiro RH. Observations on management of choledochoduodenal fistula due to penetrating peptic ulcer. Gastroenterology. 1980; 78:126–131.
Article12. Miyamoto S, Furuse J, Maru Y, Tajiri H, Muto M, Yoshino M. Duodenal tuberculosis with a choledochoduodenal fistula. J Gastroenterol Hepatol. 2001; 16:235–238.
Article13. Rutgeerts P, Onette E, Vantrappen G, Geboes K, Broeckaert L, Talloen L. Crohn's disease of the stomach and duodenum: A clinical study with emphasis on the value of endoscopy and endoscopic biopsies. Endoscopy. 1980; 12:288–294.
Article14. Min SK, Han HS, Kim EG, Kim YW, Choi YM. Laparoscopic repair of biliary-enteric fistula – report of 3 cases. J Korean Soc Endosc Laparosc Surg. 2002; 5:20–24.15. LeBlanc KA. General laparoscopic surgical complications. LeBlanc KA, editor. Management of laparoscopic surgical complications. New York: Marcel Dekker;2004. p. 43–62.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Choledocho-Duodeno-Colonic Fistula
- Cholecysto - Duodeno - Colic Fistula : Report of One Case
- Recurrent Upper Gastrointestinal Bleeding from Gastro-Cystic Fistula and Pancreatic Pseudocyst Bleeding
- Broncho-Pleuro-Gastro-Colonic Fistula: A case report
- Upper Gastrointestinal Bleeding with Cholecystoduodenal Fistula
