Laparoscopic vaginal vault closure with conventional straight instruments in single-port access total laparoscopic hysterectomy
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Bundang CHA Hospital, Seongnam, Korea.
- 2Department of Obstetrics and Gynecology, Gangnam CHA Hospital, CHA University, Seoul, Korea. yspark0108@empas.com
- 3Department of Nursing, Saekyung College, Yeongwol, Korea.
- KMID: 1500373
- DOI: http://doi.org/10.5468/ogs.2013.56.6.389
Abstract
OBJECTIVE
Laparoscopic vaginal vault closure with conventional straight instruments is the final barrier to single-port access total laparoscopic hysterectomy (SPA-TLH). The aim of this study is to find out the safer, easier, simpler, faster, and even cheaper way to overcome it.
METHODS
Vaginal vault suturing techniques of 152 consecutive single-port access total laparoscopic hysterectomy cases performed by the author in Gangnam CHA Hospital, CHA University from October 1, 2003 to June 30, 2012, were retrospectively analysed with medical records and DVDs.
RESULTS
Of 152 patients who were attempted SPA-TLH, 119 patients (78%) were finished their operations without conversion to multi-port laparoscopy or laparotomy. Of women with successful SPA-TLH, 8 cases (7%) were closed their vaginal vaults vaginally (median, 20 minutes; range, 15-44 minutes), and 111 cases (93%) laparoscopically (median, 44 minutes; range, 13-56 minutes). Laparoscopic vault closure techniques were continuous suture (4 cases, 3%; median, 36 minutes; range, 30-45 minutes), interrupted sutures using knot-pusher (7 cases, 6%; median, 52 minutes; range, 48-56 minutes) Endo Stitch suture (2 cases, 2%; median, 32 minutes; range, 13-50 minutes), continuous vault closure using percutaneous sling sutures (PCSS) (92 cases, 77%; median, 40 minutes; range, 19-56 minutes), and continuous vault closure without PCSS (6 cases, 5%; median, 23 minutes; range, 16-31 minutes).
CONCLUSION
Laparoscopic vault closure using PCSS in SPA-TLH only with conventional straight instruments is the best way to overcome the barrier and the short-cut to shorten the learning curve to date.
Keyword
Figure
-
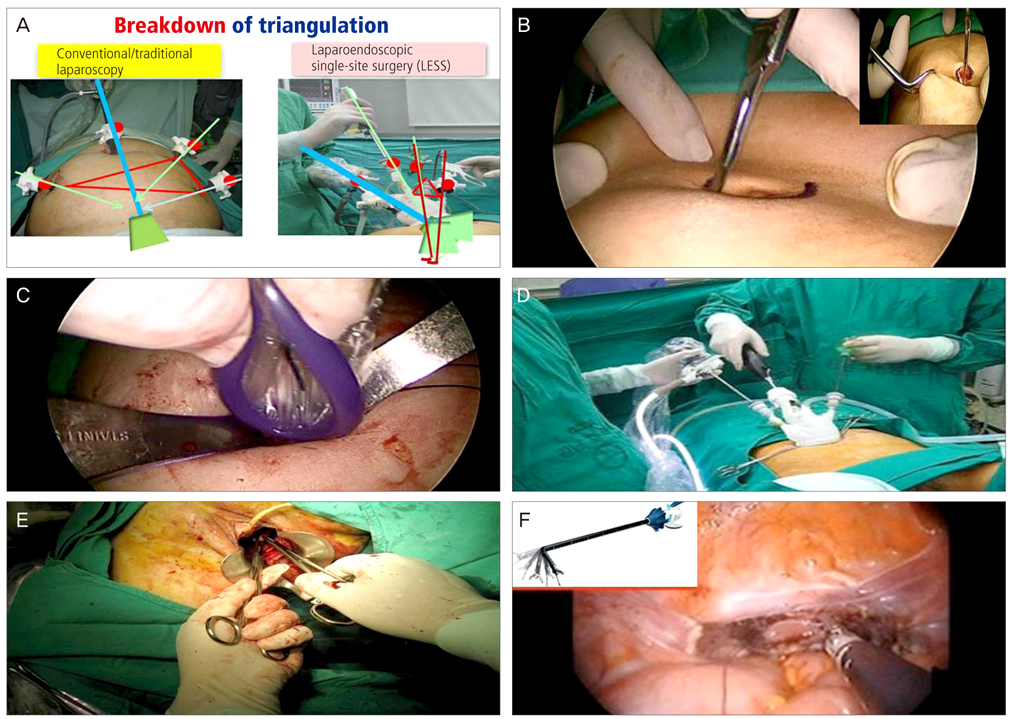
Fig. 1 (A) Breakdown of triangulation in single port access surgery. (B) Semi-lunar incision (vertical incision: left upper). (C) Insertion of Allexis retraction ring. (D) Finial view of home-made port. (E) Vaginal repair. (F) Endo Stitch suture (articulating ES: left).
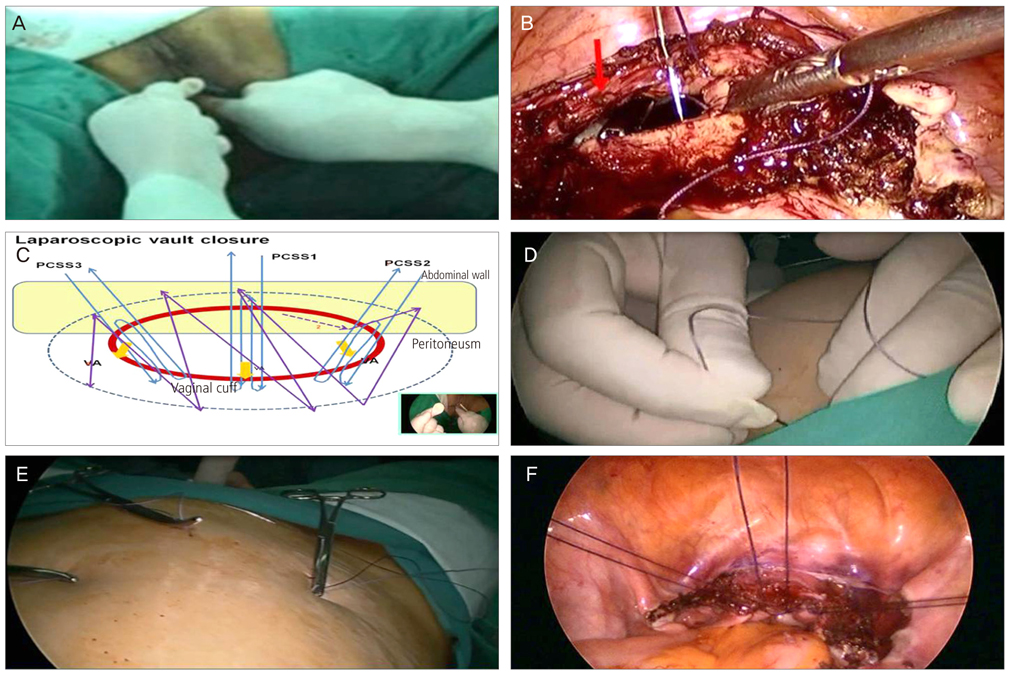
Fig. 2 (A) Vaginal manual ligation. (B) Vaginal assistance by second assistant with traumatic grasper. (C) 3 PCSS with continuous suture in SPA-TLH (schematic view). (D) Insertion of straight needle (1-0 vicryl) to abdomen. (E) Outside view of 3 PCSS. (F) Inside view of 3 PCSS in SPA-TLA. PCSS, percutaneous sling suture; SPA-TLH, single-port access total laparoscopic hysterectomy.
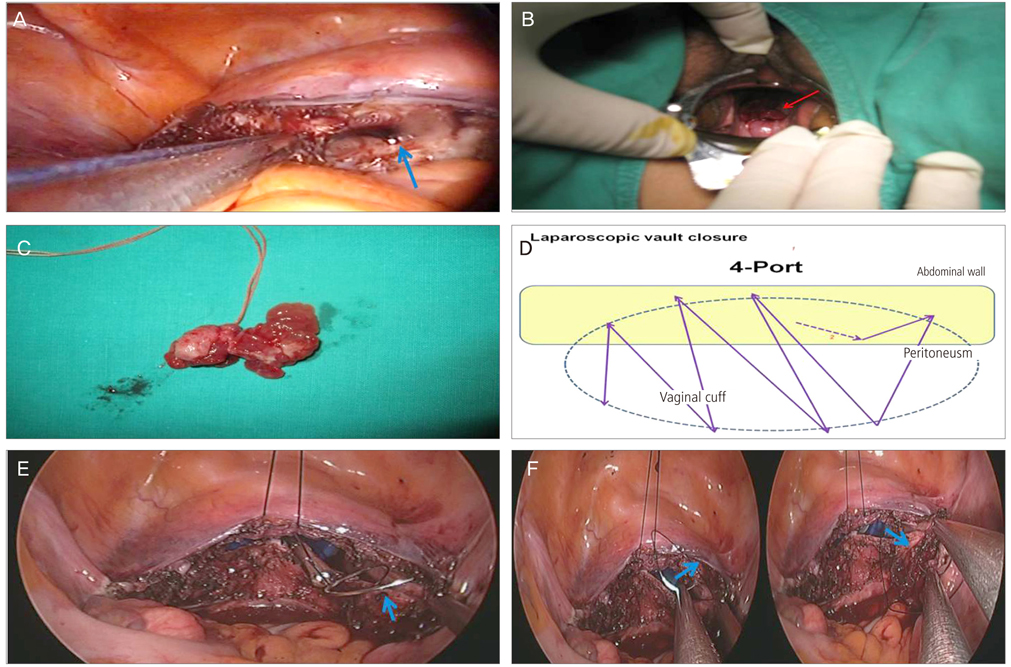
Fig. 3 (A) Extracorporeal tie with knot-pusher (arrow: vaginal assistance). (B) Vaginal vault prolapsed after SPA-TLH (salpinx). (C) Prolapsed salpinx removed after ligation. (D) Vault suture in 4-port TLH (continuous suture, schematic view). (E) Insertion of Monocryl 1-0 for vault closure (arrow: needle). (F) Continuous suture on cut-end of vesicocervical (left arrow), uterosacral (right arrow) ligament. SPA-TLH, single-port access total laparoscopic hysterectomy.
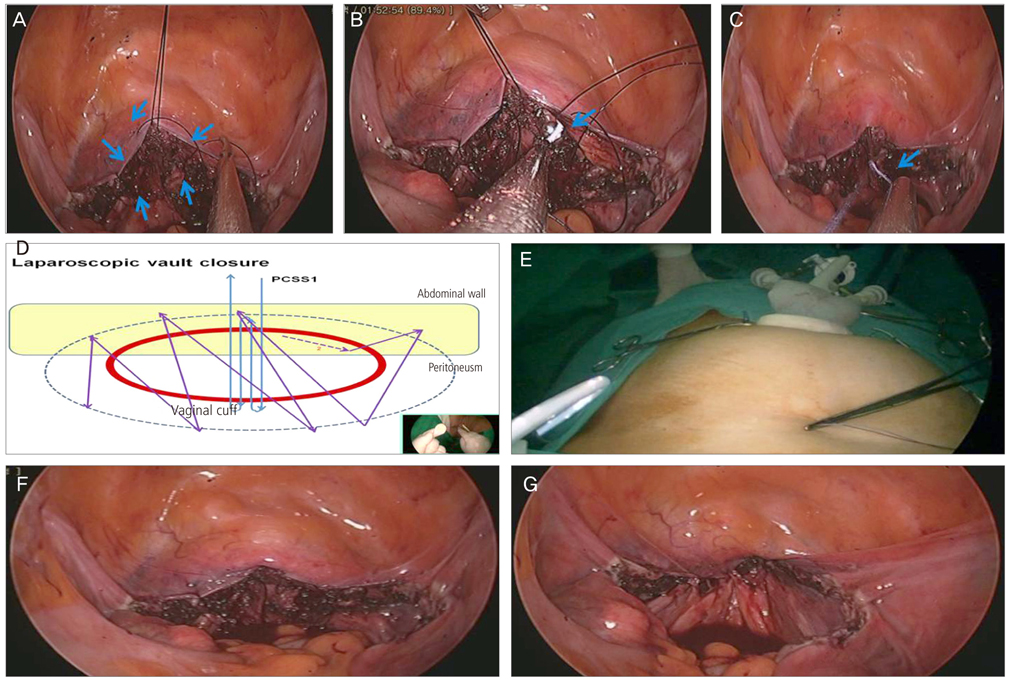
Fig. 4 (A) Continuous suture of pelvic peritoneum. (B) Retrieval of Monocryl. (C) Extracorporeal knot tying with knot-pusher. (D) 1 PCSS with continuous suture in SPA-TLH (schematic view). (E) Outside view of 1 PCSS. (F, G) View of vaginal vault before and after vaginal ligation. PCSS, percutaneous sling suture; SPA-TLH, single-port access total laparoscopic hysterectomy.
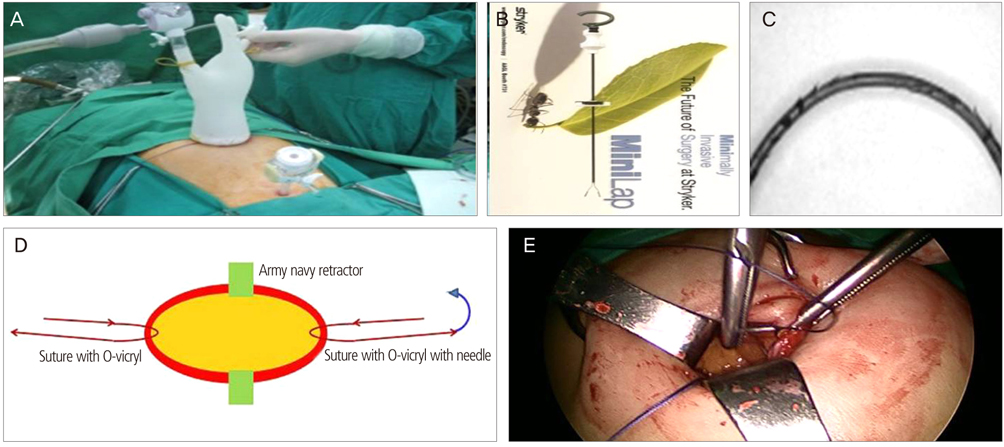
Fig. 5 (A) Outside view of 2-port laparoscopy. (B) MiniLap. (C) Barbed suture. (D) Anchoring sutures for easier port-site closure sckematic view. (E) Anchoring sutures for easier port-site closure.
Reference
-
1. Reich H, DiCaprio J, McGlynn F. Laparoscopic hysterectomy. J Gynecol Surg. 1989; 5:213–216.2. Langebrekke A, Qvigstad E. Total laparoscopic hysterectomy with single-port access without vaginal surgery. J Minim Invasive Gynecol. 2009; 16:609–611.3. Park YS. Current trends of gynecologic surgery in the 21st century: scarless surgery. Korean J Gynecol Endosc Minim Invasive Surg. 2010; 22:69–89.4. Canes D, Desai MM, Aron M, Haber GP, Goel RK, Stein RJ, et al. Transumbilical single-port surgery: evolution and current status. Eur Urol. 2008; 54:1020–1029.5. Jung YW, Kim SW, Kim YT. Recent advances of robotic surgery and single port laparoscopy in gynecologic oncology. J Gynecol Oncol. 2009; 20:137–144.6. Pelosi MA, Pelosi MA 3rd. Laparoscopic hysterectomy with bilateral salpingo-oophorectomy using a single umbilical puncture. N J Med. 1991; 88:721–726.7. Fader AN, Escobar PF. Laparoendoscopic single-site surgery (LESS) in gynecologic oncology: technique and initial report. Gynecol Oncol. 2009; 114:157–161.8. Theodoropoulou K, Lethaby DR, Bradpiece HA, Lo TL, Parihar A. Direct trocar insertion technique: an alternative for creation of pneumoperitoneum. JSLS. 2008; 12:156–158.9. Ahmad G, Duffy JM, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev. 2008; (2):CD006583.10. Tai HC, Lin CD, Wu CC, Tsai YC, Yang SS. Homemade transumbilical port: an alternative access for laparoendoscopic single-site surgery (LESS). Surg Endosc. 2010; 24:705–708.11. Park YS. Total laparoscopic hysterectomy: self-study. Seoul: Gabon Med Co.;2008.12. Park D, Jeong H. Vaginal vault evisceration after total laparoscopic hysterectomy. Korean J Gynecol Endosc Minim Invasive Surg. 2012; 24:120–126.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of 110 cases of single-port access laparoscopically assisted vaginal hysterectomy (SPA-LAVH) and comparison with multi-port access
- Single port transumbilical total laparoscopic hysterectomy (TLH): initial experience in Korea
- Techniques of gynecologic single-port access laparoscopic surgery
- Three cases of vaginal evisceration after laparoscopic hysterectomy
- Single port access laparoscopic myomectomy
