Traumatic Lumbosacral Spinal Subdural Hematoma Mimicking Subdural Lipoma: Value of Computed Tomography
- Affiliations
-
- 1Department of Orthopaedic Surgery, Gyeongsang National University School of Medicine, Jinju, Korea. dhkim8311@gnu.ac.kr
- 2Department of Anesthesiology, Gyeongsang National University School of Medicine, Jinju, Korea.
- 3Department of Radiology, Gyeongsang National University School of Medicine, Jinju, Korea.
- 4Research Institute of Clinical Medicine, Gyeongsang National University School of Medicine, Jinju, Korea.
- 5Institute of Health Sciences, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 1494153
- DOI: http://doi.org/10.4055/jkoa.2013.48.5.397
Abstract
- Traumatic lumbosacral spinal subdural hematoma due to anatomical and pathological causes is rare, compared to epidural hematoma. If the time of trauma cannot be determined, intracranial and intraspinal signal intensity according to lapse of time are not coincident, resulting in confusion in terms of differentiation. Fat suppression magnetic resonance image (MRI) and computed tomography (CT) are utilized for differentiation. The intention of this study is to report on a case where spinal subdural hematoma of unknown time of occurrence is differentiated from subdural lipoma by taking advantage of fat suppression MRI and CT in order to perform an early surgical decompression with auxiliary review of literature demonstrating good prognosis of the procedure.
MeSH Terms
Figure
-

Figure 1 Preoperative radiographs. (A) Posteroanterior and (B) lateral plain radiographs showed endplate sclerotic changes and osteophytes of the lumbar spine.

Figure 2 (A) T1 weight image sagittal magnetic resonance image (MRI) demonstrating a hyperintense signal (B) T2 weight image sagittal MRI demonstrating an intermediate to low signal from L1 to S2 level suggestive of a subdural hematoma causing thecal sac compression (arrows). Axial (C) T1 and (D) T2-weighted MRI showing signal intensity, correlating with an early subacute subdural hematoma at the anterior and posterior location of the spinal canal (asterisk points: 'inverted Mercedes sign').
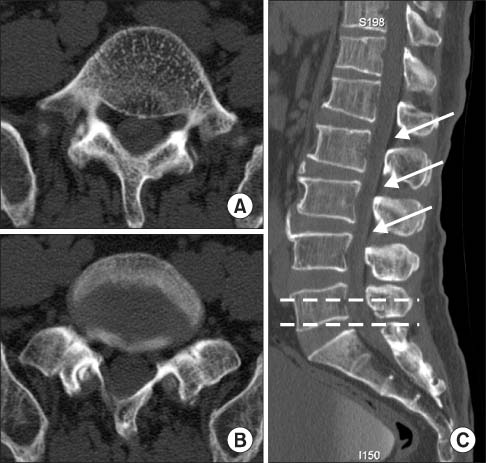
Figure 3 Preoperative computed tomography (A: upper doted line on C, B: lower doted line on C) different axial level view and (C) sagittal view showing differences in signal density between the hematoma (isodensity) and epidural fat (low density, arrows).

Figure 4 (A) Lumbar 4-5 level puncture. (B) Hematoma mixed with cerebrospinal fluid was aspirated by 3 ml.
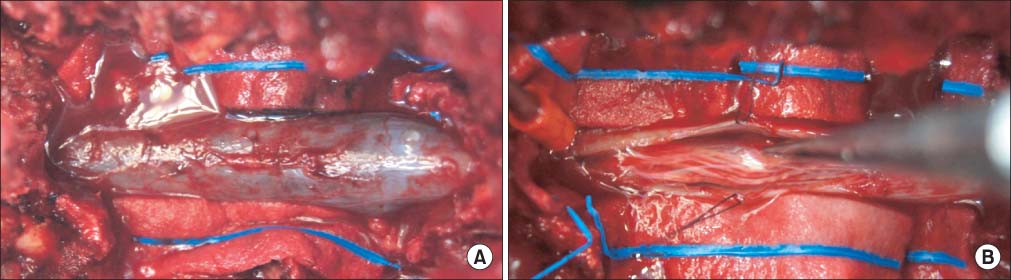
Figure 5 (A) After total laminectomy of L4 and L5, a dark-reddish transparent hematoma was observed beneath the dura. (B) Bleeding was observed around the right L4 root which may be considered a valveless radiculomedullary vein, and it was coagulated with bipolar bovie.
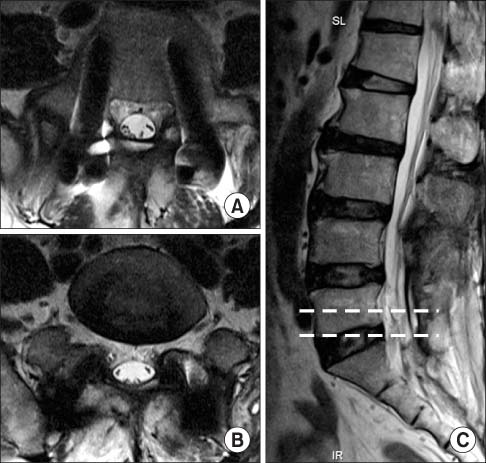
Figure 6 Magnetic resonance images taken three months after surgery (A: upper doted line on C, B: lower doted line on C). T2-weight axial images demonstrate recovery of normal signal density without thecal sac compression. (C) T2-weight sagittal image showing disappearance of the subdural hematoma.
Reference
-
1. Diyora B, Sharma A, Mamidanna R, Kamat L. Chronic cervicothoracic spinal subdural hematoma. Neurol Med Chir (Tokyo). 2009; 49:310–312.2. Rader JP. Chronic subdural hematoma of the spinal cord: report of a case. N Engl J Med. 1955; 253:374–376.3. Russell NA, Benoit BG. Spinal subdural hematoma. A review. Surg Neurol. 1983; 20:133–137.
Article4. Hung KS, Lui CC, Wang CH, Wang CJ, Howng SL. Traumatic spinal subdural hematoma with spontaneous resolution. Spine (Phila Pa 1976). 2002; 27:E534–E538.
Article5. Mavroudakis N, Levivier M, Rodesch G. Central cord syndrome due to a spontaneously regressive spinal subdural hematoma. Neurology. 1990; 40:1306–1308.
Article6. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: a literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003; 26:1–49.
Article7. Johnson PJ, Hahn F, McConnell J, Graham EG, Leibrock LG. The importance of MRI findings for the diagnosis of nontraumatic lumbar subacute subdural haematomas. Acta Neurochir (Wien). 1991; 113:186–188.
Article8. Braun P, Kazmi K, Nogués-Meléndez P, Mas-Estellés F, Aparici-Robles F. MRI findings in spinal subdural and epidural hematomas. Eur J Radiol. 2007; 64:119–125.
Article9. Kamo M, Watanabe Y, Numaguchi Y, Saida Y. Spinal subdural hematoma mimicking epidural lipomatosis. Magn Reson Med Sci. 2012; 11:197–199.
Article10. Post MJ, Becerra JL, Madsen PW, et al. Acute spinal subdural hematoma: MR and CT findings with pathologic correlates. AJNR Am J Neuroradiol. 1994; 15:1895–1905.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Spinal Subdural Hematoma Accompanying intracranial hematoma: Spontaneous Resolution after Pumbar Puncture
- Intraoperative Development of Contralateral Subdural Hematoma during Evacuation of Acute Subdural Hematoma: Case Report
- Acute-on-chronic subdural hematoma by spinal anesthesia in a patient with undiagnosed chronic subdural hematoma: A case report
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Clinical Evaluation of the Traumatic Subdural Hygroma
