Clin Exp Otorhinolaryngol.
2008 Jun;1(2):113-115. 10.3342/ceo.2008.1.2.113.
Chemocauterization of Congenital Fistula from the Accessory Parotid Gland
- Affiliations
-
- 1Department of Otorhinolaryngology, Seoul National University College of Medicine, Seoul, Korea. jhunhah@snu.ac.kr
- KMID: 1486064
- DOI: http://doi.org/10.3342/ceo.2008.1.2.113
Abstract
- Congenital sialo-cutaneous fistula arising from the accessory parotid gland is extremely rare. Although the fistula tract can be successfully excised after making a skin incision along the skin tension line around the fistula opening, a facial scar inevitably remains. We here report a case of sialo-cutaneous fistula that was treated with chemocauterization with trichloroacetic acid (TCA). TCA cauterization is an easy and effective option for the treatment of congenital fistula from an accessory parotid gland, especially from the aesthetic point of view.
Keyword
Figure
-
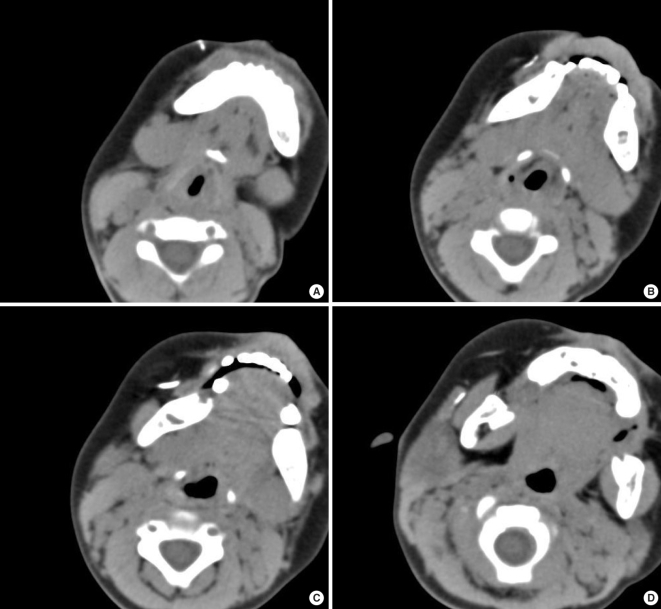
Fig. 1 Initial findings of CT-sialography. (A-D) Fistula tract from the outside opening of the right anterior cheek to the accessory gland at the anterior aspect of the right parotid gland.

Fig. 2 Chemocauterization of a sialo-cutaneous fistula with trichloroacetic acid (TCA) solution. (A) Intraoperative findings. A small metal suction tip was inserted through the fistula opening. A lacrimal probe, held by a surgeon, indicated the end of the suction tip. The length of the fistula tract was about 6 cm. Two mL of 40% TCA solution was injected for chemocauterization of the tract. (B) Postoperative findings after 2 month. The fistula opening was completely closed and only a small dimple remained. The cosmetic result was very satisfactory.
Reference
-
1. Currarino G, Votteler TP. Lesions of the accessory parotid gland in children. Pediatr Radiol. 2006; 1. 36(1):1–7. PMID: 16284760.
Article2. Frommer J. The human accessory parotid gland: its incidence, nature, and significance. Oral Surg Oral Med Oral Pathol. 1977; 5. 43(5):671–676. PMID: 266146.
Article3. Yamasaki H, Tashiro H, Watanabe T. Congenital parotid gland fistula. Int J Oral Maxillofac Surg. 1986; 8. 15(4):492–494. PMID: 3091733.
Article4. Jernstrom P, Prietto CA. Accessory parotid gland tissue at base of neck. Arch Pathol. 1962; 6. 73:473–480. PMID: 14451707.5. Moon WK, Han MH, Kim IO, Sung MW, Chang KH, Choo SW, et al. Congenital fistula from ectopic accessory parotid gland: diagnosis with CT sialography and CT fistulography. AJNR Am J Neuroradiol. 1995; 4. 16(4 Suppl):997–999. PMID: 7611095.6. Kim KH, Sung MW, Koh TY, Oh SH, Kim IS. Pyriform sinus fistula: management with chemocauterization of the internal opening. Ann Otol Rhinol Laryngol. 2000; 5. 109(5):452–456. PMID: 10823473.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lessons From a Case of Failed Attempt to Remove Pleomorphic Adenoma of the Accessory Parotid Gland via Transoral Approach
- Pleomorphic adenoma in accessory salivary gland: A case report
- Surgical Treatment of Primary and Metastatic Malignant Tumors of the Accessory Parotid Gland
- 6 Cases of Salivary Gland Tumors Arising at Buccal and Masseteric Area
- A Case of Parotid Gland Salivary Fistula Treated by Tympanic Neurectomy
