Bone Transport Over the Intramedullary Nail for Defects of Long Bone
- Affiliations
-
- 1Department of Orthopedic Surgery, National Medical Center, School of Medicine, Korea University, Seoul, Korea.
- 2Department of Orthopedic Surgery, School of Medicine, Kyungpook National University, Daegu, Korea. cwoh@knu.ac.kr
- KMID: 1480962
- DOI: http://doi.org/10.12671/jkfs.2008.21.1.37
Abstract
-
PURPOSE: To evaluate the results of bone transport using external fixator over an intramedullary nail for defects of long bone.
MATERIALS AND METHODS
We treated 14 cases of bone defect after chronic osteomyelitis or trauma of tibia (12 cases) and femur (2 cases) using this method. The mean age of index procedure was 46.9 years, and all of them had follow-up study for a mean of 3 years. After the corticotomy and insertion of intramedullary nail, bone transport was done by external fixators. Then, the segment was moved and bone graft was done at docking site.
RESULTS
The mean transported amount was 5.8 cm, and the external fixator was removed after 141 days. The mean external fixation index was 25.6 days/cm. Primary union of distraction and docking site was achieved in all, but one had failure in union of docking site. According to the Mekhail's functional criteria, there were 5 excellent, 6 good, and 3 fair results. Among 15 complications, there were 2 major complications with residual sequelae, and they were 1 recurred osteomyelitis and 1 flexion contracture of knee.
CONCLUSION
Bone transport using external fixator over an intramedullary nail, can successfully solve defects of long bone. Since this method can remove external fixators earlier than the conventional method, it has fewer complications and makes patients to return to daily life earlier.
MeSH Terms
Figure
-

Fig. 1 (A) The patient had a large bone defect of 12 cm after the operation of tibial osteomyelitis. (B, C) With the insertion of intramedullary nail, ilizarov ring fixator was fixed to transport the distal segment.

Fig. 2 (A) After the transport, bone graft was done on the docking site with plate fixation. (B, C) At two years of follow-up, the tibia was well reconstructed without leg length discrepancy.
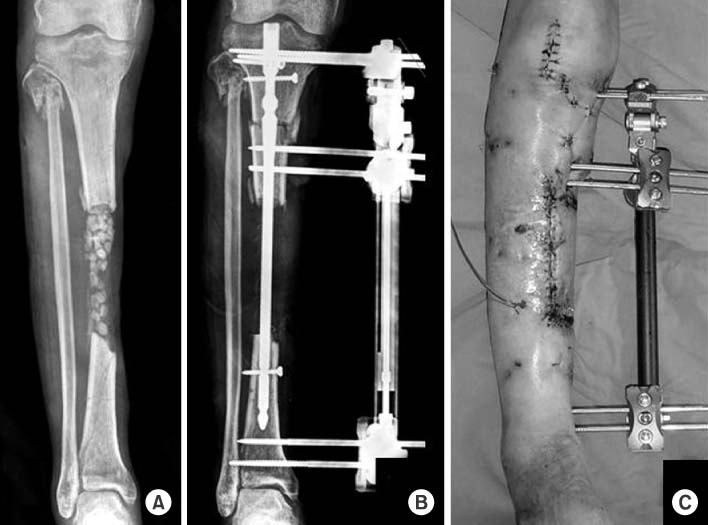
Fig. 3 (A) The patient showed a large tibial bone loss with the insertion of antibiotic cement-beads. (B, C) Proximal corticotomy was done for transport by the methods of external fixator over the intramedullary nail.

Fig. 4 (A) Bone graft was done on the docking site. (B) The distracted callus was good in consolidation at 3 month. (C) At the final follow-up, the tibia was well reconstructed.

Fig. 5 After the traumatic bone loss of the proximal tibia (A), external fixation was done over the intramedullary nail. Note the posterior angulation of proximal tibia (B). Bone transport was done from the distal fragment (C), and bone graft was made on the docking site.

Fig. 6 The external fixator was removed at 2 month after bone graft (A). At two years of follow-up, the tibia was well reconstructed. Although the knee joint shows procurvatum with anterior angulation of proximal tibia (B, C), the patient had a good functional outcome.
Cited by 2 articles
-
Treatment for Bone Defect of Open Tibial Fractures by Using Intramedullary Nail Fixation with Autogenous Iliac Bone Graft
Hyub Sakong, Ki Cheor Bae, Chul Hyun Cho, Kyung Jae Lee, Eun Seok Son, Du Han Kim
J Korean Fract Soc. 2012;25(4):288-294. doi: 10.12671/jkfs.2012.25.4.288.Treatment for Bone Defect of Open Tibial Fractures by Using Intramedullary Nail Fixation with Autogenous Iliac Bone Graft
Hyub Sakong, Ki Cheor Bae, Chul Hyun Cho, Kyung Jae Lee, Eun Seok Son, Du Han Kim
J Korean Fract Soc. 2012;25(4):288-294. doi: 10.12671/jkfs.2012.25.4.288.
Reference
-
1. Aronson J, Johnson E, Harp JH. Local bone transportation for treatment of intercalary defects by the Ilizarov technique. Biomechanical and clinical considerations. Clin Orthop Relat Res. 1989; 243:71–79.2. Cattaneo R, Catagni M, Johnson EE. The treatment of infected nonunions and segmental defects of the tibia by the methods of Ilizarov. Clin Orthop Relat Res. 1992; 280:143–152.
Article3. Cierny G 3rd, Zorn KE. Segmental tibial defects. Comparing conventional and Ilizarov methodologies. Clin Orthop Relat Res. 1994; 301:118–123.4. Dagher F, Roukoz S. Compound tibial fractures with bone loss treated by the Ilizarov technique. J Bone Joint Surg Br. 1991; 73:316–321.
Article5. Dendrinos GK, Kontos S, Lyritsis E. Use of the Ilizarov technique for treatment of non-union of the tibia associated with infection. J Bone Joint Surg Am. 1995; 77:835–846.
Article6. Freedman EL, Johnson EE. Radiographic analysis of tibial fracture malalignment following intramedullary nailing. Clin Orthop Relat Res. 1995; 315:25–33.
Article7. Green SA. Skeletal defects. A comparison of bone grafting and bone transport for segmental skeletal defects. Clin Orthop Relat Res. 1994; 301:111–117.
Article8. Hofmann GO, Gonschorek O, Buhren V. Segment transport employing intramedullary devices in tibial bone defects following trauma and infection. J Orthop Trauma. 1999; 13:170–177.
Article9. Ilizarov GA. Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res. 1990; 250:8–26.
Article10. Kwon CS, Kim YW, Jung BH, Shin KS. The treatment of infected nonunoins of the tibia by the methods of Ilizarov. J Korean Soc Fract. 1995; 8:347–353.
Article11. Marsh JL, Prokuski L, Biermann JS. Chronic infected tibial nonunions with bone loss. Conventional techniques versus bone transport. Clin Orthop Relat Res. 1994; 301:139–146.12. Mekhail AO, Abraham E, Gruber B, Gonzalez M. Bone transport in the management of posttraumatic bone defects in the lower extremity. J Trauma. 2004; 56:368–378.
Article13. Oh CW, Min WK, Kyung HS, et al. Internal bone transport in the management of tibial bone defects. J Korean Fract Soc. 2005; 18:36–42.
Article14. Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res. 1990; 250:81–104.
Article15. Paley D, Catagni MA, Argnani F, Villa A, Benedetti GB, Cattaneo R. Ilizarov treatment of tibial non-unions with bone loss. Clin Orthop Relat Res. 1989; 241:146–165.
Article16. Paley D, Herzenberg JE, Paremain G, Bhave A. Femoral lengthening over an intramedullary nail: a matched-case comparison with Ilizarov lengthening. J Bone Joint Surg Am. 1997; 79:1464–1480.17. Paley D, Maar DC. Ilizarov bone transport treatment for tibial defects. J Orthop Trauma. 2000; 14:76–85.
Article18. Polyzois D, Papachristou G, Kotsiopoulos K, Plessas S. Treatment of tibial and femoral bone loss by distraction osteogenesis: experience in 28 infected and 14 clean cases. Acta Orthop Scand Suppl. 1997; 275:84–88.19. Ring D, Jupiter JB, Gan BS, Israeli R, Yaremchuk MJ. Infected nonunion of the tibia. Clin Orthop Relat Res. 1999; 369:302–311.
Article20. Song HR, Kale A, Park HB, et al. Comparison of internal bone transport and vascularized fibular grafting for femoral bone defects. J Orthop Trauma. 2003; 17:203–211.
Article21. Song HR, Oh CW, Mattoo R, et al. Femoral lengthening over an intramedullary nail using the external fixator: risk of infection and knee problems in 22 patients with a follow-up of 2 years or more. Acta Orthop. 2005; 76:245–252.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Difficulty in Removal of a Femoral Intramedullary Nail: The Geometry of the Distal End of the Nail
- Retrieval of a Broken Intramedullary Nail after Refracture of Femoral Shaft: A case report
- Comparison of Intramedullary Nailing and Plate Fixation for the Treatment of Nonunion of the Long Bone Fracture on Lower Extermities
- Thermal Injury Complicating Improperly Reamed Intramedullary Nailing of the Tibia: A Case Report
- Bone Density and Mechanical Property after Locked Intramedullary Nailing of the Long Bone Fractures: Preliminary Study of QCT & Lunar of 15 Long Bone Fractures
