Recurrent Postoperative Effusive-Constrictive Pericarditis Associated with Steroid Discontinuation
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jksong@amc.seoul.kr
- KMID: 1473735
- DOI: http://doi.org/10.4250/jcu.2009.17.3.102
Abstract
- Transient effusive-constrictive pericarditis is a rare complication of open-heart surgery, but is increasingly recognized. For patients with both pericardial effusion and constrictive physiology soon after uneventful open-heart surgery, proper treatment remains to be established. We experienced a case of transient effusive-constrictive pericarditis in a 50-year-old woman who underwent aortic valve replacement due to infective endocarditis. Initially, she was treated with both prednisolone and ibuprofen, which resulted in dramatic relief of symptom. However, she suffered from a relapse of pericaridis after rapid steroid discontinuation and was stabilized by re-treatment with steroid.
MeSH Terms
Figure
-
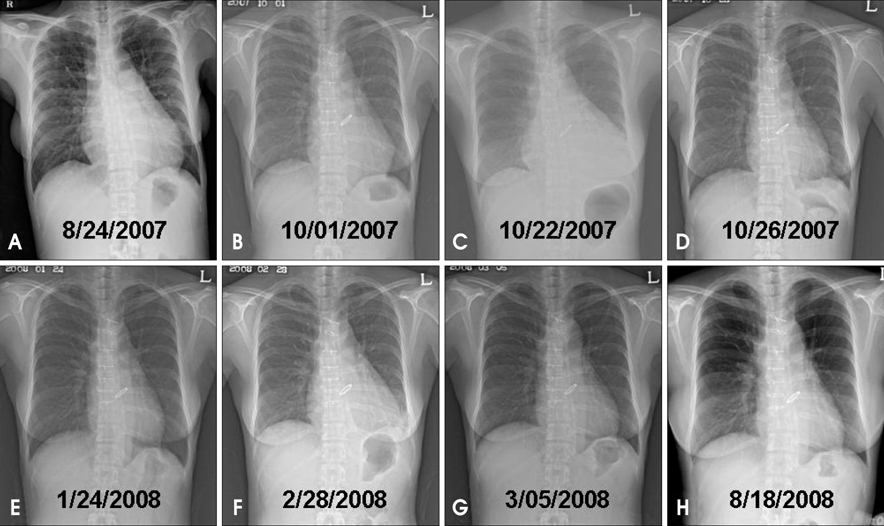
Fig. 1 A series of chest X-ray. Preoperative chest X-ray showed moderate cardiomegaly with increased pulmonary vascularity (A). Cardiomegaly and pulmonary congestion after operation was resolved (B). In 8 weeks after surgery, chest X-ray showed aggravated cardiomegaly compared with previous one (C). Under the diagnosis of postoperative effusive-constrictive pericarditis, patient was treated with prednisolone and ibuprofen for 7 weeks. Chest X-ray showed normalized heart size within 1 week (D) and after treatment (E). In 3 months after steroid discontinuation, chest X-ray revealed cardiomegaly again (F). The patient was suspected as recurrent effusive-constrictive pericarditis potentially associated with steroid discontinuation. Chest X-ray showed normalized heart size within 1 week (G) and in 6 months (H) after re-treatment with steroid.

Fig. 2 Representative echocardiograms. Preoperative transesophageal echocardiography showed multiple vegetations attached to aortic valve (A). After uneventful aortic valve replacement, moderate pericardial effusion (PE) with typical constrictive physiology developed (B and C), which resolved dramatically with medical treatment (D). After steroid discontinuation, pericardial effusion (E) and constrictive physiology redeveloped (F). Asterisk: vegetations.
Reference
-
1. Sagristà-Sauleda J, Permanyer-Miralda G, Candell-Riera J, Angel J, Soler-Soler J. Transient cardiac constriction: an unrecognized pattern of evolution in effusive acute idiopathic pericarditis. Am J Cardiol. 1987. 59:961–966.
Article2. Oh JK, Hatle LK, Mulvagh SL, Tajik AJ. Transient constrictive pericarditis: diagnosis by two-dimensional Doppler echocardiography. Mayo Clin Proc. 1993. 68:1158–1164.
Article3. Haley JH, Tajik AJ, Danielson GK, Schaff HV, Mulvagh SL, Oh JK. Transient constrictive pericarditis: causes and natural history. J Am Coll Cardiol. 2004. 43:271–275.
Article4. Yang HS, Song JK, Song JM, Kang DH, Lee CW, Nam GB, Choi KJ, Kim YH, Hong MK, Kim JJ, Park SW, Park SJ, Song H, Lee JW, Song MG. Clinical characteristics of constrictive pericarditis diagnosed by echo-Doppler technique in Korea. J Korean Med Sci. 2001. 16:558–566.
Article5. Finkelstein Y, Shemesh J, Mahlab K, Abramov D, Bar-El Y, Sagie A, Sharoni E, Sahar G, Smolinsky AK, Schechter T, Vidne BA, Adler Y. Colchicine for the Prevention of Postpericardiotomy Syndrome. Herz. 2002. 27:791–794.
Article6. Cha KS, Young YB, Ahn YK, Park JC, Seo JP, Park JH, Jeong MH, Cho JG, Park JC, Kang JC. Postoperative effusive constrictive pericarditis in ventricular septal defect repair. J Korean Soc Echocardiogr. 1997. 5:36–41.
Article7. Imazio M, Trinchero R, Shabetai R. Pathogenesis, management, and prevention of recurrent pericarditis. J Cardiovasc Med (Hagerstown). 2007. 8:404–410.
Article8. Imazio M, Bobbio M, Cecchi E, Demarie D, Demichelis B, Pomari F, Moratti M, Gaschino G, Giammaria M, Ghisio A, Belli R, Trinchero R. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation. 2005. 112:2012–2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Effusive-Constrictive Pericarditis in and Infant Treated by Pericardiectomy
- Clinical Studies on Acute Pericarditis with Effusion and Chronic Constrictive Pericarditis with or without Effusion
- Postoperative Effusive Constrictive Pericarditis in Ventricular Septal Defect Repair
- A case of delayed appearance of effusive-constrictive pericarditis after radiation therapy for Hodgkin's disease
- Constrictive Pericarditis Following Acute Idiopathic Pericarditis
