Extensive Primary Cardiac Lymphoma Diagnosed by Percutaneous Endomyocardial Biopsy
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, St. Mary's Hospital, Seoul, Korea. younhj@catholic.ac.kr
- KMID: 1473718
- DOI: http://doi.org/10.4250/jcu.2009.17.4.141
Abstract
- Primary cardiac lymphoma (PCL) is an extranodal non-Hodgkin's lymphoma exclusively located in the heart and/or pericardium. It is rare in immunocompetent patients and represents 1.3% of primary cardiac tumors and 0.5% of extranodal lymphomas. The clinical behavior is aggressive and the early symptoms are cardiac failure, syncope, arrhythmia, or pericardial effusion. Although echocardiography, computed tomography (CT) scan, magnetic resonance image (MRI) are the mainly used imaging techniques to detect cardiac tumors, pathologic examination is always required to confirm the diagnosis. Diagnosis of PCL is difficult due to non-specific clinical manifestations and requires invasive approach to get histopathologic evidence. While surgery with systemic chemotherapy or in combination with irradiation has been attempted, the only effective treatment is chemotherapy. However, the prognosis remains poor. We report on a 42-year-old woman who is diagnosed histopathologically as PCL by cardiac catheterization assisted percutaneous endomyocardial biopsy and treated successfully by anthracycline based chemotherapy.
MeSH Terms
Figure
-
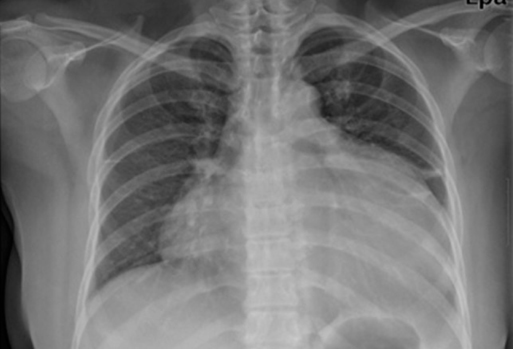
Fig. 1 Chest radiography demonstrates marked cardiomegaly with globular shape of heart.
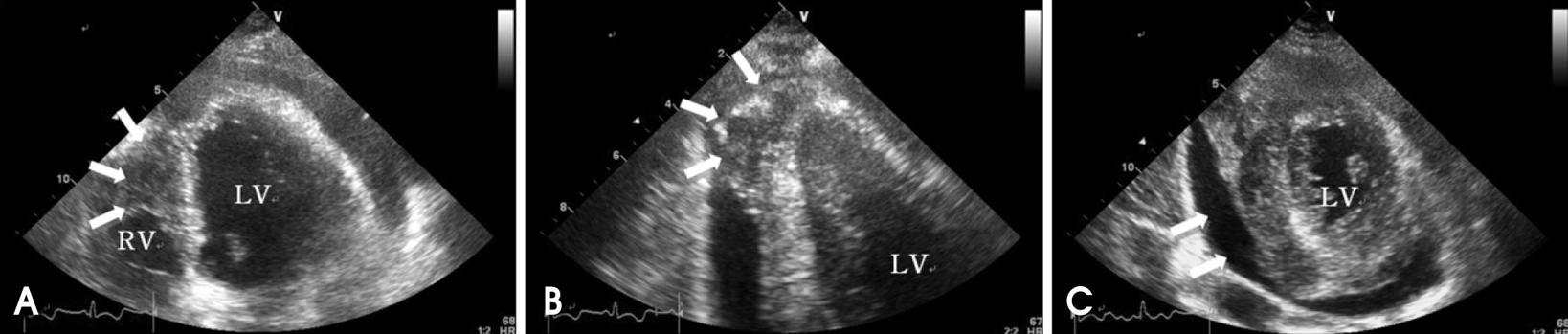
Fig. 2 A: Apical 4 chamber view demonstrates infiltrative tumor mass in RV apical cavity (white arrow). B: On apical 2 chamber view, protruding mass (white arrow) is observed in LV apex with moderate amount of pericardial effusion. C: Parasternal short axis view at the mid-ventricular level shows moderate amount of pericardial effusion (white arrow) and mass in posteroinferior LV myocardium. LV: left ventricle, RV: right ventricle.
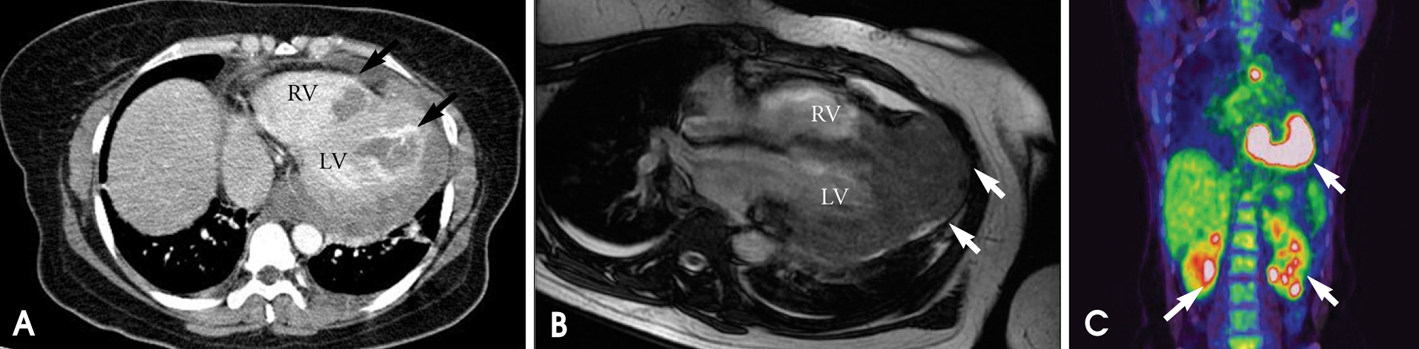
Fig. 3 A: Computed tomography reveals intracardiac mass involving both ventricles (black arrow). B: Magnetic resonance imaging (MRI) demonstrates mass on LV base which extended from pericardium to RV and LV (white arrow). C: PET/CT revealing malignant tumor involving the LV, RV and pericardial region as well as intense FDG uptake at LA and left lower paratracheal region and both kidneys. LV: left ventricle, RV: right ventricle, PET/CT: positron emission tomography/computed tomography, FDG: fluorodeoxyglucose, LA: left atrium.
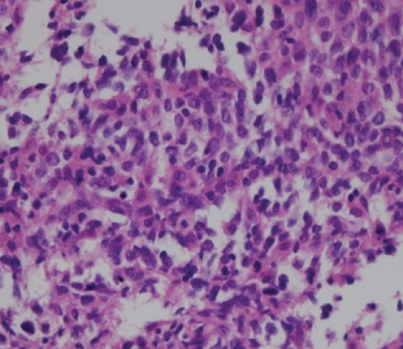
Fig. 4 High power view of the left ventricular endomyocardial tumor. The tumor cells are atypical lymphocytes regarded as lymphoma cells. Hematoxylin and eosin stain (×100).
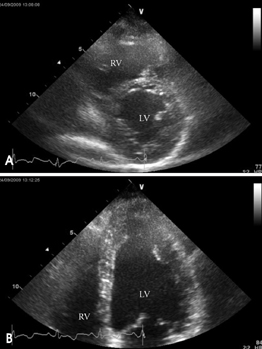
Fig. 5 A: Parasternal short axis view at the mid-ventricular level shows no more observed tumor mass and pericardial effusion. B: On apical 4 chamber view, there is no infiltrating cardiac mass in LV and RV apex. LV: left ventricle, RV: right ventricle.
Reference
-
1. Piccaluga PP, Vigna E, Placci A, Agostinelli C, Laterza C, Papayannidis C, Leone O, Martinelli G, Zinzani PL, Baccarani M, Pileri SA. Primary cardiac non-Hodgkin lymphoma presenting with atrial flutter and pericardial effusion. Br J Haematol. 2006. 134:356.
Article2. Chalabreysse L, Berger F, Loire R, Devouassoux G, Cordier JF, Thivolet-Bejui F. Primary cardiac lymphoma in immunocompetent patients: a report of three cases and review of the literature. Virchows Arch. 2002. 441:456–461.
Article3. Utsunomiya D, Awai K, Urata J, Hirayama T, Yamashita Y. Primary cardiac lymphoma: computed tomography and magnetic resonance imaging features. Jpn J Radiol. 2009. 27:243–246.
Article4. Anghel G, Zoli V, Petti N, Remotti D, Feccia M, Pino P, Majolino I. Primary cardiac lymphoma: report of two cases occurring in immunocompetent subjects. Leuk Lymphoma. 2004. 45:781–788.
Article5. Motto A, Ballo P, Zito D, Cadenotti L, Moroni M, Dessanti P, Fedeli F. Primary cardiac lymphoma presenting as sick sinus syndrome. J Clin Oncol. 2008. 26:6003–6005.
Article6. Nascimento AF, Winters GL, Pinkus GS. Primary cardiac lymphoma: clinical, histologic, immunophenotypic, and genotypic features of 5 cases of a rare disorder. Am J Surg Pathol. 2007. 31:1344–1350.
Article7. Zaharia L, Gill PS. Primary cardiac lymphoma. Am J Clin Oncol. 1991. 14:142–145.
Article8. Ryu SJ, Choi BW, Choe KO. CT and MR findings of primary cardiac lymphoma: report upon 2 cases and review. Yonsei Med J. 2001. 42:451–456.
Article9. Ceresoli GL, Ferreri AJ, Bucci E, Ripa C, Ponzoni M, Villa E. Primary cardiac lymphoma in immunocompetent patients: diagnostic and therapeutic management. Cancer. 1997. 80:1497–1506.
Article10. Higo T, Takemoto M, Ogawa K, Inoue S, Eshima K, Tada H, Sunagawa K. Intracardiac echocardiography-guided cardiac tumor biopsy. Circ J. 2009. 73:381–383.
Article11. Jang EH, Kim WS, Kim ST, Kang JH, Park GW, Jung CW, Park KC. Primary cardiac lymphoma presented as 3 degree AV block and right ventricular failure. Korean J Intern Med. 2006. 70:341–346.12. Park KS, Ahn WS, Lee S, Kwon OC, Ko MS, Jheon SH. Primary non-Hodgkin's lymphoma in right ventricle with right atrial invasion. Report of 1 case. Korean J Thorac Cardiovasc Surg. 2004. 37:376–381.13. Kim JY, Woo CM, Lee JY, Lee JB, Ryu JK, Choi JY, Chang SG, Shin JH, Lee WS, Seo JH, Kim YS. A case of primary cardiac non-Hodgkin's lymphoma. Korean Cir J. 2004. 34:808–812.
Article14. Kang SB, Jin SW, Lee EK, Park YH, Choi YH, Kim YK, Park JC. A case of non-Hodgkin's lymphoma with massive involvement of the right atrium. Korean Cir J. 2000. 30:492–496.
Article15. Choi WS, Han IY, Jun HJ, Lee YH, Hwang YH, Cho KH. Primary malignant cardiac lymphoma in right atrium. A case report. Korean J Thorac Cardiovasc Surg. 2008. 41:369–372.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multimodality Imaging Can Help to Doubt, Diagnose and Follow-Up Cardiac Mass
- Primary Cardiac Lymphoma: Case Report
- Long-term disease-free survival of patients with primary cardiac lymphoma treated with systemic chemotherapy and radiotherapy
- Primary Non-Hodgkin's Lymphoma in Right Ventricle with Right Atrial Invasion: Report of 1 case
- Diffuse Infiltrative Primary Cardiac Lymphoma with Delayed Extracardiac Involvement
