J Cardiovasc Ultrasound.
2009 Dec;17(4):138-140. 10.4250/jcu.2009.17.4.138.
Pulmonary Valve Endocarditis with Septic Pulmonary Thromboembolism in a Patient with Ventricular Septal Defect
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul National University College of Medicine, Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea. cardioch@medimail.co.kr
- 2Division of Cardiology, Department of Internal Medicine, Seoul National University College of Medicine, Seoul National University Hospital, Seoul, Korea.
- KMID: 1473717
- DOI: http://doi.org/10.4250/jcu.2009.17.4.138
Abstract
- We describe a 42-year-old man who presented as life-threatening sepsis and septic shock with multiple septic pulmonary embolism and septic pneumonia due to pulmonary valve endocarditis. The patient had history of untreated ventricular septal defect (VSD) and complained of severe dyspnea and orthopnea. Transthoracic and transesophageal echocardiograms revealed severe pulmonary regurgitation with large, hypermobile vegetation on pulmonary valve and right ventricular outflow tract (RVOT), and a small subarterial type VSD. Emergency operation was done due to rapid deterioration of the patient, and after 6 weeks of antibiotics coverage, he was discharged.
MeSH Terms
Figure
-
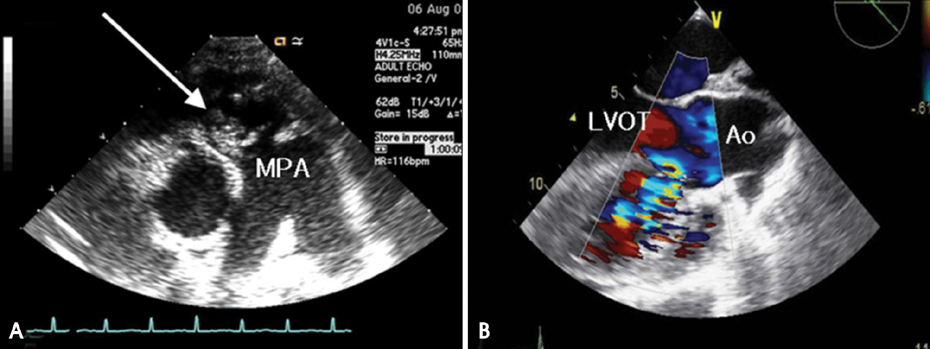
Fig. 1 A: Transthoracic parasternal short axis view showing large, mobile vegetation (white arrow) on pulmonary valve. B: Transesophageal echocardiography showing a small subarterial type VSD with left to right shunt. Large amount of thrombus and vegetation were found in right ventricle. MPA: main pulmonary artery, LVOT: left ventricular outflow tract, Ao: aorta.

Fig. 2 Initial chest CT showing (A) pulmonary embolism (white arrows) and (B) destructed pulmonary valve (white arrows). Lung parenchyme on CT shows diffuse grass ground opacity with multifocal patchy and nodular consolidations at both lungs suggesting combined septic pneumonia.
Reference
-
1. Berlin JA, Abrutyn E, Strom BL, Kinman JL, Levison ME, Korzeniowski OM, Feldman RS, Kaye D. Incidence of infective endocarditis in the Delaware Valley, 1988-1990. Am J Cardiol. 1995. 76:933–936.
Article2. Hogevik H, Olaison L, Andersson R, Lindberg J, Alestig K. Epidemiologic aspects of infective endocarditis in an urban population. A 5-year prospective study. Medicine (Baltimore). 1995. 74:324–339.
Article3. Ha JK, Kim SH, Kim SH, An BJ, Chun KJ, Hong TJ, Shin YW, Chung SW, Kim JW. Infected endocarditis related pacemaker leads: a case report. J Korean Soc Echocardiogr. 2001. 9:70–74.
Article4. Tariq M, Smego RA Jr, Soofi A, Islam N. Pulmonic valve endocarditis. South Med J. 2003. 96:621–623.
Article5. Nishida K, Fukuyama O, Nakamura DS. Pulmonary valve endocar-ditis caused by right ventricular outflow obstruction in association with sinus of valsalva aneurysm: a case report. J Cardiothorac Surg. 2008. 3:46.
Article6. Moyssakis I, Kazazis A, Lionakis N, Vlahodimitris I, Petrikos G, Votteas V. Late recurrence of pulmonic valve endocarditis in an adult patient with ventricular septal defect: a case report. J Heart Valve Dis. 2009. 18:167–169.7. Nakauchi Y, Taniguchi M, Miyamura Y, Ishise T, Miyazaki S. [Pulmonary septic embolism with right side infectious endocarditis and ventricular septal defect: a case report.]. J Cardiol. 2007. 50:383–387.8. Ali AA, Halstead JC, Hosseinpour AR, Ali ZA, Kumar S, Wallwork J. Replacement of a regurgitant pulmonary valve with a stentless bioprosthesis. Ann Thorac Surg. 2004. 78:1467–1468.
Article9. Ramadan FB, Beanlands DS, Burwash IG. Isolated pulmonic valve endocarditis in healthy hearts: a case report and review of the literature. Can J Cardiol. 2000. 16:1282–1288.10. Kim SH, Woo HY, Ha JH, Kim WC, Choi YS, Rhee DH, Kim JH, Park CS, Oh YS, Youn HJ, Chung WS, Hong SJ. A case of patent ductus arteriosus associated with pulmonary valve endocarditis. J Cardiovasc Ultrasound. 2006. 14:33–35.
Article11. Musci M, Siniawski H, Pasic M, Grauhan O, Weng Y, Meyer R, Yankah CA, Hetzer R. Surgical treatment of right-sided active infective endocarditis with or without involvement of the left heart: 20-year single center experience. Eur J Cardiothorac Surg. 2007. 32:118–125.
Article12. Melina G, El-Hamamsy I, Sinatra R, Yacoub MH. Late fulminant pulmonary valve endocarditis after the Ross operation. J Thorac Cardiovasc Surg. 2009. Inpress.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Thromboembolism and Infarction Caused by Right-Sided Infective Endocarditis in a Patient with Ventricular Septal Defect
- A Case Report of Ventricular Septal Defect with Bacterial Endocarditis and Pulmonic Valve Vegetation
- A Case of Septic Pulmonary Emboli in Ventricular Septal Defect
- Clinical and Echocardiographic Features of Pulmonic Valve Endocarditis in patients with Ventricular Septal Defect
- Two Cases of Pulmonic Valvular Vegetation and Pulmonary Infarction Associated with VSD
