Korean J Hepatobiliary Pancreat Surg.
2013 Aug;17(3):109-112. 10.14701/kjhbps.2013.17.3.109.
Technical knacks and outcomes of extended extrahepatic bile duct resection in patients with mid bile duct cancer
- Affiliations
-
- 1Division of Hepatobiliary Surgery and Liver Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- KMID: 1472525
- DOI: http://doi.org/10.14701/kjhbps.2013.17.3.109
Abstract
- BACKGROUNDS/AIMS
Mid bile duct cancers often involve the proximal intrapancreatic bile duct, and resection of the extrahepatic bile duct (EHBD) can result in a tumor-positive distal resection margin (RM). We attempted a customized surgical procedure to obtain a tumor-free distal RM during EHBD resection, so that R0 resection can be achieved without performing pancreaticoduodenectomy through extended EHBD resection.
METHODS
We previously reported the surgical procedures of extended EHBD resection, in which the intrapancreatic duct excavation resembles a > or =2 cm-long funnel. This unique procedure was performed in 11 cases of mid bile duct cancer occurring in elderly patients between the ages of 70 and 83 years.
RESULTS
The tumor involved the intrapancreatic duct in all cases. Deep pancreatic excavation per se required about 30-60 minutes. Cancer-free hepatic duct RM was obtained in 10 patients. Prolonged leakage of pancreatic juice occurred in 2 patients, but all were controlled with supportive care. Adjuvant therapies were primarily applied to RM-positive or lymph node-positive patients. Their 1-year and 3-year survival rates were 90.9% and 60.6%, respectively.
CONCLUSIONS
We suggest that extended EHBD resection can be performed as a beneficial option to achieve R0 resection in cases in which pancreaticoduodenectomy should be avoided due to various causes including old age and expectation of a poor outcome.
MeSH Terms
Figure
-
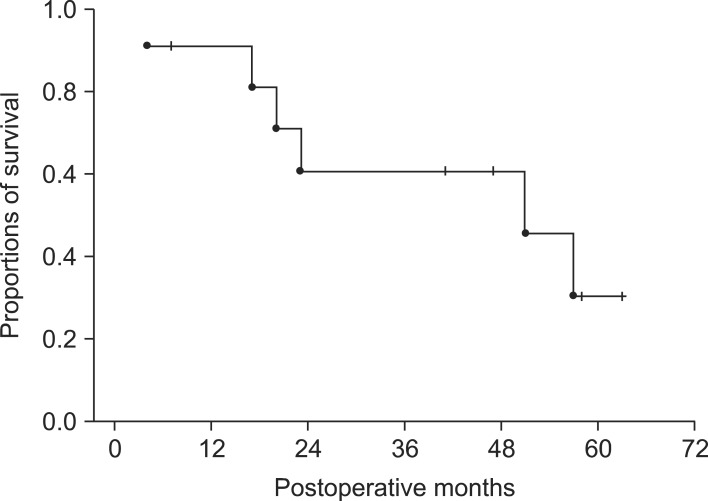
Fig. 1 Survival outcomes of 11 mid bile duct cancer patients who underwent extended extrahepatic bile duct resection.
Cited by 1 articles
-
Retroduodenal resection of the extrahepatic common bile duct with in situ re-implantation of the main pancreatic duct: A report of two cases
Shin Hwang, Dong-Hwan Jung, Tae-Yong Ha
Ann Hepatobiliary Pancreat Surg. 2020;24(3):373-380. doi: 10.14701/ahbps.2020.24.3.373.
Reference
-
1. Stein DE, Heron DE, Rosato EL, et al. Positive microscopic margins alter outcome in lymph node-negative cholangiocarcinoma when resection is combined with adjuvant radiotherapy. Am J Clin Oncol. 2005; 28:21–23. PMID: 15685030.
Article2. Oh D, Lim do H, Heo JS, et al. The role of adjuvant radiotherapy in microscopic tumor control after extrahepatic bile duct cancer surgery. Am J Clin Oncol. 2007; 30:21–25. PMID: 17278890.
Article3. Hwang S, Lee SG, Kim KH, et al. Extended extrahepatic bile duct resection to avoid performing pancreatoduodenectomy in patients with mid bile duct cancer. Dig Surg. 2008; 25:74–79. PMID: 18292664.
Article4. Seyama Y, Kubota K, Kobayashi T, et al. Two-staged pancreatoduodenectomy with external drainage of pancreatic juice and omental graft technique. J Am Coll Surg. 1998; 187:103–105. PMID: 9660033.
Article5. Shimada H, Endo I, Fujii Y, et al. Procedure of extended hilar bile duct resection and its application for hilar cholangiocarcinoma. Hepatogastroenterology. 2002; 49:300–305. PMID: 11995438.6. Murakami Y, Uemura K, Hayashidani Y, et al. Prognostic significance of lymph node metastasis and surgical margin status for distal cholangiocarcinoma. J Surg Oncol. 2007; 95:207–212. PMID: 17278119.
Article7. Ebata T, Watanabe H, Ajioka Y, et al. Pathological appraisal of lines of resection for bile duct carcinoma. Br J Surg. 2002; 89:1260–1267. PMID: 12296893.
Article8. Wakai T, Shirai Y, Moroda T, et al. Impact of ductal resection margin status on long-term survival in patients undergoing resection for extrahepatic cholangiocarcinoma. Cancer. 2005; 103:1210–1216. PMID: 15685618.
Article9. Bhuiya MR, Nimura Y, Kamiya J, et al. Clinicopathologic factors influencing survival of patients with bile duct carcinoma: multivariate statistical analysis. World J Surg. 1993; 17:653–657. PMID: 8273388.
Article10. Nagorney DM, Donohue JH, Farnell MB, et al. Outcomes after curative resections of cholangiocarcinoma. Arch Surg. 1993; 128:871–877. PMID: 8393652.
Article11. Todoroki T, Kawamoto T, Koike N, et al. Treatment strategy for patients with middle and lower third bile duct cancer. Br J Surg. 2001; 88:364–370. PMID: 11260100.
Article12. Kayahara M, Nagakawa T, Ohta T, et al. Role of nodal involvement and the periductal soft-tissue margin in middle and distal bile duct cancer. Ann Surg. 1999; 229:76–83. PMID: 9923803.
Article13. Sakamoto Y, Kosuge T, Shimada K, et al. Prognostic factors of surgical resection in middle and distal bile duct cancer: an analysis of 55 patients concerning the significance of ductal and radial margins. Surgery. 2005; 137:396–402. PMID: 15800484.
Article14. Hirono S, Tani M, Kawai M, et al. Indication of hepatopancreatoduodenectomy for biliary tract cancer. World J Surg. 2006; 30:567–573. PMID: 16568228.
Article15. D'Angelica M, Martin RC 2nd, Jarnagin WR, et al. Major hepatectomy with simultaneous pancreatectomy for advanced hepatobiliary cancer. J Am Coll Surg. 2004; 198:570–576. PMID: 15051011.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extrahepatic Bile Duct Duplication with Intraductal Papillary Neoplasm: A Case Report
- Clinical Review of Carcinomas of the Extrahepatic Bile Ducts and Gallbladders
- Recurrent pyogenic cholangitis: The pattern of thickening of the extrahepatic bile duct on CT
- A Case of Multiple Papillary Adenocarcinoma of the Extrahepatic Bile Duct : Findings of ERCP
- Concurrent Yellow-to-white and Black Extrahepatic Bile Duct Stones
