A Successful Primary Percutaneous Coronary Intervention Twelve Days After a Cabrol Composite Graft Operation in Marfan Syndrome
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea. jojeong@cnu.ac.kr
- 2Department of Radiology, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea.
- KMID: 1456371
- DOI: http://doi.org/10.4070/kcj.2010.40.5.247
Abstract
- The Cabrol procedure is one of several techniques used for re-implantation of a coronary artery. After replacement of the ascending aorta and aortic valve using a composite graft, second Dacron tube grafts are used for anastomosis between the ascending aortic graft and the coronary arteries. Ostial stenosis is one of the complications associated with the Cabrol operation. However, there have been no reported cases of acute thrombosis of a Cabrol graft. Here we report a case with acute ST elevation myocardial infarction due to thrombotic total occlusion of a right Cabrol graft-to-right coronary artery (RCA) twelve days after surgery in a patient with Marfan syndrome. He was successfully treated with primary percutaneous coronary intervention (PCI).
MeSH Terms
Figure
-

Fig. 1 This coronary angiogram taken twelve days after the Cabrol graft operation revealed total occlusion by thrombi at the Cabrol graft to the right coronary artery anastomosis site (A: white arrow). After ballooning of the anastomosis site, it revealed a narrowed, angulated, and twisted distal limb of the graft anastomosis site (B). The coronary angiogram after stent implantation revealed complete reopening of the Cabrol graft to the right coronary artery (C).

Fig. 2 Initial intravascular ultrasound and schematic illustrations showed a kinked and narrowed anastomotic site (A and B). After stent deployment, it showed optimal lesion coverage (C and D).
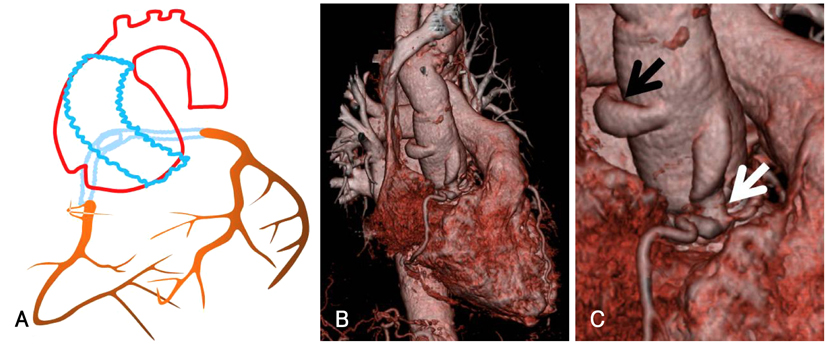
Fig. 3 Schematic illustration of the Cabrol procedure showed that after replacement of the ascending aorta and aortic valve using a composite graft, a second Dacron tube graft is used to connect the ascending aortic graft and the coronary arteries (A). Coronary CT angiography shows that the left limb (black arrow) and the right limb of the Cabrol graft (white arrow) was kinked and narrowed at the anastomotic site (B and C).
Reference
-
1. Bachet J, Termignon JL, Goudot B, et al. Aortic root replacement with a composite graft: factors influencing immediate and long-term results. Eur J Cardiothorac Surg. 1996. 10:207–213.2. Midulla PS, Ergin A, Galla J, et al. Three faces of the Bentall procedure. J Card Surg. 1994. 9:466–481.3. Kurisu K, Ochiai Y, Kajiwara T, Kumeda H, Tominaga R. A modified valve-on-valve approach for aortic root replacement. Ann Thorac Surg. 2003. 76:2099–2101.4. Gelsomino S, Frassani R, Da Col P, et al. A long-term experience with the Cabrol root replacement technique for the management of ascending aortic aneurysms and dissections. Ann Thorac Surg. 2003. 75:126–131.5. Murakami T, Senoo Y, Teramoto S. Long-term results with total replacement of the ascending aorta and aortic valve. Kyobu Geka. 1991. 44:8 Suppl. 697–701.6. Cabrol C, Pavie A, Gandjbakhch I, et al. Complete replacement of the ascending aorta with reimplantation of the coronary arteries: new surgical approach. J Thorac Cardiovasc Surg. 1981. 81:309–315.7. Witzenbichler B, Schwimmbeck P, Schultheiss HP. Images in cardiovascular medicine: myocardial infarction caused by occlusion of Cabrol conduit graft. Circulation. 2005. 112:e79–e80.8. Coram R, George Z, Breall JA. Percutaneous intervention through a Cabrol composite graft. Catheter Cardiovasc Interv. 2005. 66:356–359.9. Wells TA, Kapoor A. Percutaneous coronary intervention through a Cabrol composite graft. Int J Cardiol. 2007. 116:e44–e45.10. Hussain F, Ducas J, Gosal T. Emergent percutaneous intervention with a drug-eluting stent of a Cabrol graft-to-left main anastomosis during a non-ST-elevation infarction in a patient with Marfan's syndrome. J Invasive Cardiol. 2006. 18:E250–E252.11. Koh KG, Hyon MS, Lim HJ, et al. Cardiovascular manifestations of Marfan syndrome. Korean Circ J. 1987. 17:777–782.12. Guak KO, Kang JC, Ryoo JY, Lee YH, Hwang YH, Cho KH. Early and midterm results of Cabrol technique in the aortic root replacement. Korean J Thorac Cardiovasc Surg. 2000. 33:547–551.13. Kim JW, Lee JT, Cho JY, Kim KT, Kim GJ. The results of using the Cabrol technique for aortic root replacement. Korean J Thorac Cardiovasc Surg. 2008. 41:573–579.14. Baek MJ, Na CY, Kim WH, et al. Composite graft aortic root replacement with coronary button reimplantation: the early and mid-term results. Korean J Thorac Cardiovasc Surg. 2002. 35:356–364.15. Cetin G, Tireli E, Ozkara A, Suzer K. Occlusion and stenosis of coronary perfusion graft after reconstruction of ascending aorta with the Cabrol technique. Eur J Cardiothorac Surg. 2004. 25:284–285.16. Guilmet D, Bonnet N, Saal JP, Le Houerou D, Ghorayeb G. Long term survival with the Bentall button operation in 150 patients. Arch Mal Coeur Vaiss. 2004. 97:83–91.17. Mestres CA, Betriu A, Pomar JL. Occlusion of the coronary perfusion graft: an exceptional complication after reconstruction of the ascending aorta with the Cabrol technique. J Thorac Cardiovasc Surg. 1989. 98:302–303.18. Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Composite valve graft replacement of the proximal aorta: comparison of techniques in 348 patients. Ann Thorac Surg. 1992. 54:427–439.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Advances in Percutaneous Coronary Intervention in Coronary Artery Disease
- True Aneurysm of the Common Coronary Button in a Marfan Patient with an Anomalous Right Coronary Artery after a Bentall Procedure: A Case Report
- Right coronary artery atresia in Marfan's syndrome: A case report
- A Case of a Successful Percutaneous Coronary Intervention Using Percusurge(r) System in a Massive Intracoronary Thrombi Patient
- Staged versus One-Time Percutaneous Coronary Intervention Strategy for Multivessel Non-ST Segment Elevation Acute Coronary Syndrome
