Pulmonary Metastasis from Rectal Cancer on Chest CT Is Correlated with 3T MRI Primary Tumor Location
- Affiliations
-
- 1Department of Radiology, Anam Hospital, Korea University College of Medicine, Seoul, Korea. dr.minjukim@gmail.com
- KMID: 1443479
- DOI: http://doi.org/10.3348/jksr.2011.65.2.151
Abstract
- PURPOSE
To evaluate the association between the incidence of pulmonary metastasis on chest CT and the location of the primary tumor on rectal MRI.
MATERIALS AND METHODS
One hundred and nine consecutive patients with rectal adenocarcinoma underwent chest CT and 3T rectal MRI. Two radiologists classified the tumor on MRI as an upper (> 10 cm from the anal verge), mid (5-10 cm), or lower rectal tumor (< 5 cm) by consensus. All chest CT scans were retrospectively reviewed for the presence of metastasis. We used Fisher's exact test to evaluate the correlation between the incidence of pulmonary metastasis with the location of the rectal cancer and the Mantel-Haenszel test to control for local tumor stage.
RESULTS
We only included the 60 patients with upper (n = 26) or lower (n = 34) rectal cancer, because of the complicated venous drainage system of the mid rectum. Among these, 9 (15%) showed evidence of pulmonary metastasis on chest CT and almost all (89%, 8/9) patients had lower rectal cancer. The incidence of pulmonary metastasis between the two groups was statistically different (p < 0.05) when local tumor stage was controlled.
CONCLUSION
The incidence of pulmonary metastasis was significantly higher for lower than upper rectal cancers when the T-stage of the tumor was accounted for.
MeSH Terms
Figure
-
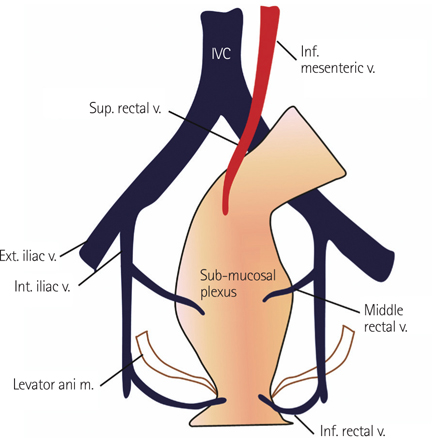
Fig. 1 Anatomy of the rectal venous plexus. The rectum has two drainage veins. The upper and middle thirds of the rectum drain primarily into the superior rectal vein and finally empty into the liver via the inferior mesenteric vein and portal vein. However, the lower third of the rectum drains into the middle rectal vein. The blood in the middle rectal vein skips the liver because it drains directly into the IVC. Note.-IVC = inferior vena cava

Fig. 2 The method used to determine the location of the tumor. A patient with a mid rectal tumor (arrowhead). On the sagittal T2-weighted image, a line (dotted line) was drawn along the midline of the rectal lumen and then another two lines (solid lines) were drawn vertically at the level of the lower margin of the tumor and the anal verge. The distance from the lower margin of the tumor to the anal verge was measured in a zigzag pattern (double-headed arrows).
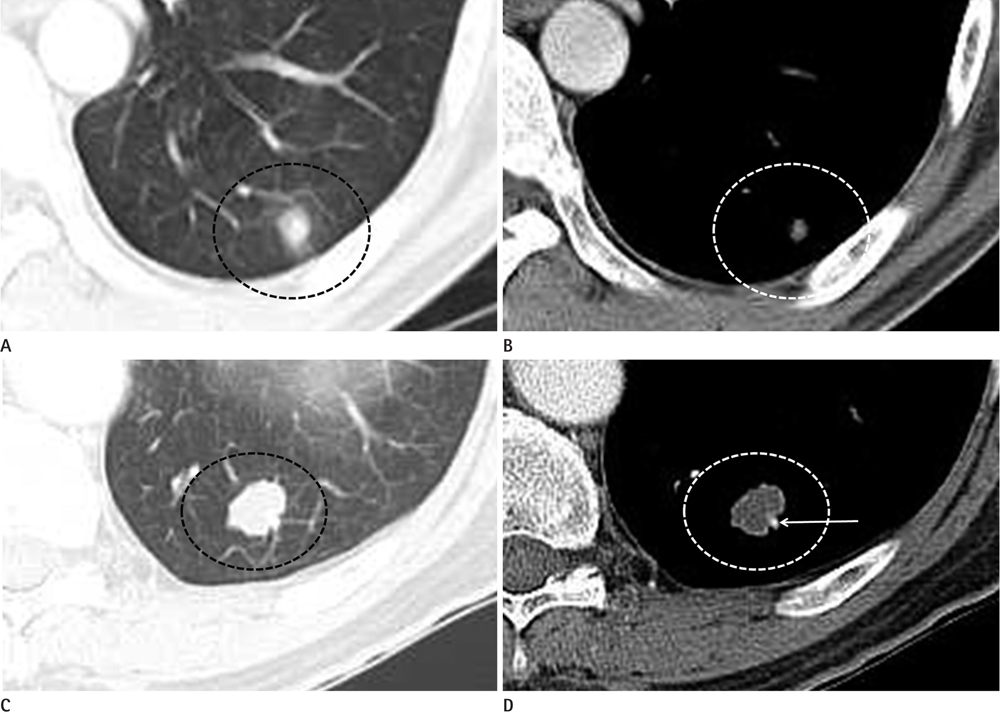
Fig. 3 Chest CT scans of two patients who were considered to have pulmonary metastases. Chest CT scans with the lung (A) and mediastinum (B) setting of a 37-year-old man with rectal adenocarcinoma. A nodule (dotted circles) measuring about 0.9 cm in size without calcification was detected. Another nodule larger than 0.5 cm in diameter was also detected (not shown), and therefore, this patient was considered to have pulmonary metastasis. Chest CT scans with the lung (C) and mediastinum (D) setting of a 69-year-old man with rectal adenocarcinoma. A nodule (dotted circle) measuring about 1.9 cm in size without calcification in diameter is visible. The nodule was determined to be a metastatic lesion. The hyperdense dot beside the nodule (arrow) is a nearby enhanced pulmonary artery.

Fig. 4 Selection of patients for the study. Of the 109 patients considered, 2 were excluded because the measured distance to the anal verge was over 15 cm. Of the 107 patients, 34 patients and a lower rectal tumor, 47 had a mid rectal tumor, and 26 had an upper rectal tumor. Of the 15 patients who had chest CT scans suspicious for lung metastasis, 8 had a primary rectal tumor, 6 had a mid rectal tumor, while 1 had an upper rectal tumor. The patients with a mid rectal tumor were excluded from the statistical analyses because of the complexity of the venous drainage of the mid rectum.
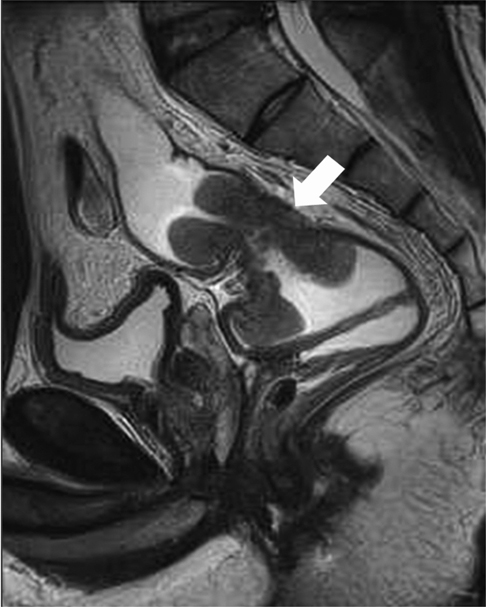
Fig. 5 A 34-year-old man with rectal adenocarcinoma. The sagittal T2-weighted image shows a pedunculated rectal mass (arrow). The shape of the mass and more uncommonly, the acute angled and dilated rectum makes it difficult to determine the location of the tumor.
Reference
-
1. Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Park EC, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2008. Cancer Res Treat. 2011; 43:1–11.2. Tan KK, Lopes Gde, Sim R. How uncommon are isolated lung metastases in colorectal cancer? A review from database of 754 patients over 4 years. J Gastrointest Surg. 2009; 13:642–648.3. Parnaby CN, Bailey W, Balasingam A, Beckert L, Eglinton T, Fife J, et al. Pulmonary staging in colorectal cancer: a review. Colorectal Dis. 2012.4. Sakamoto T, Tsubota N, Iwanaga K, Yuki T, Matsuoka H, Yoshimura M. Pulmonary resection for metastases from colorectal cancer. Chest. 2001; 119:1069–1072.5. Welton ML, Pineda CE, Chang GJ, Shelton AA. Anorectum. In : Doherty GM, editor. Current Diagnosis & Treatment: surgery. 13th ed. New York: McGraw-Hill;2009. p. 698–723.6. Zhang XM, Zhang HL, Yu D, Dai Y, Bi D, Prince MR, et al. 3-T MRI of rectal carcinoma: preoperative diagnosis, staging, and planning of sphincter-sparing surgery. AJR Am J Roentgenol. 2008; 190:1271–1278.7. Taylor FG, Swift RI, Blomqvist L, Brown G. A systematic approach to the interpretation of preoperative staging MRI for rectal cancer. AJR Am J Roentgenol. 2008; 191:1827–1835.8. Kirke R, Rajesh A, Verma R, Bankart MJ. Rectal cancer: incidence of pulmonary metastases on thoracic CT and correlation with T staging. J Comput Assist Tomogr. 2007; 31:569–571.9. Grossmann I, Avenarius JK, Mastboom WJ, Klaase JM. Preoperative staging with chest CT in patients with colorectal carcinoma: not as a routine procedure. Ann Surg Oncol. 2010; 17:2045–2050.10. Kosmider S, Stella DL, Field K, Moore M, Ananda S, Oakman C, et al. Preoperative investigations for metastatic staging of colon and rectal cancer across multiple centres--what is current practice? Colorectal Dis. 2009; 11:592–600.11. Kronawitter U, Kemeny NE, Heelan R, Fata F, Fong Y. Evaluation of chest computed tomography in the staging of patients with potentially resectable liver metastases from colorectal carcinoma. Cancer. 1999; 86:229–235.12. McIntosh J, Sylvester PA, Virjee J, Callaway M, Thomas MG. Pulmonary staging in colorectal cancer--is computerised tomography the answer? Ann R Coll Surg Engl. 2005; 87:331–333.13. Van Cutsem E, Oliveira J. ESMO Guidelines Working Group. Primary colon cancer: ESMO clinical recommendations for diagnosis, adjuvant treatment and follow-up. Ann Oncol. 2009; 20:Suppl 4. 49–50.14. National Comprehensive Cancer Network (U.S.). Clinical Practice Guidelines in Oncology - v.2. 2009. [CD-ROM]. Rockledge: NCCN;2009.15. Penna C, Nordlinger B. Colorectal metastasis (liver and lung). Surg Clin North Am. 2002; 82:1075–1090. x–xi.16. Barlow AD, Nakas A, Pattenden C, Martin-Ucar AE, Dennison AR, Berry DP, et al. Surgical treatment of combined hepatic and pulmonary colorectal cancer metastases. Eur J Surg Oncol. 2009; 35:307–312.17. McAfee MK, Allen MS, Trastek VF, Ilstrup DM, Deschamps C, Pairolero PC. Colorectal lung metastases: results of surgical excision. Ann Thorac Surg. 1992; 53:780–785. discussion 785-786.18. Kim CK, Kim SH, Chun HK, Lee WY, Yun SH, Song SY, et al. Preoperative staging of rectal cancer: accuracy of 3-Tesla magnetic resonance imaging. Eur Radiol. 2006; 16:972–980.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endotracheal Metastasis Seen on FDG PET/CT in a Patient with Previous Colorectal Cancer
- The Role of Preoperative Chest CT in the Evaluation of a Colorectal Adenocarcinoma
- Interpretation of Rectal MRI after Neoadjuvant Treatment in Patients with Rectal Cancer
- Diagnostic Performance of Rectal CT for Staging Rectal Cancer: Comparison with Rectal MRI and Histopathology
- Predictive value of chest computed tomography for axillary lymph node metastasis in patients with breast cancer A retrospective cohort study
