The Role of Diffusion-Weighted MRI in Differentiation of Idiopathic Acute Transverse Myelitis and Acute Spinal Cord Infarction
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea. joonwoo2@gmail.com
- 2Department of Neurology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 1443470
- DOI: http://doi.org/10.3348/jksr.2011.65.2.101
Abstract
- PURPOSE
To compare the diffusion characteristics of idiopathic acute transverse myelitis (ATM) and acute spinal cord infarction (SCI).
MATERIALS AND METHODS
Diffusion-weighted images (DWI) and an apparent diffusion coefficient (ADC) map were prospectively obtained from patients diagnosed with myelopathy between February 2006 and April 2009. Inclusion criteria included 1) the presence of an intramedullary T2-high signal intensity and 2) a final diagnosis of idiopathic ATM or SCI established by one neurologist. In total, 13 patients (M : F = 8 : 5; mean age, 39.5 years; range, 29-50 years) with idiopathic ATM and seven patients (M : F = 2 : 5; mean age, 58 years; range, 48-75 years) with SCI were included in this study. Two radiologists evaluated the DWIs and ADC map in consensus. The extent of the cord signal change was also evaluated on T2-weighted sagittal images.
RESULTS
Among the 16 patients with ATM, 14 patients showed iso-signal on an ADC map, but one case showed restricted diffusion and another showed increased diffusion on the ADC map. Among the seven patients with SCI, five patients showed restricted diffusion.
CONCLUSION
Idiopathic ATM usually does not demonstrate restricted diffusion, which can be a clue to differentiate it from SCI. However, idiopathic ATM with larger segment involvement can show focal diffusion restriction.
MeSH Terms
Figure
-
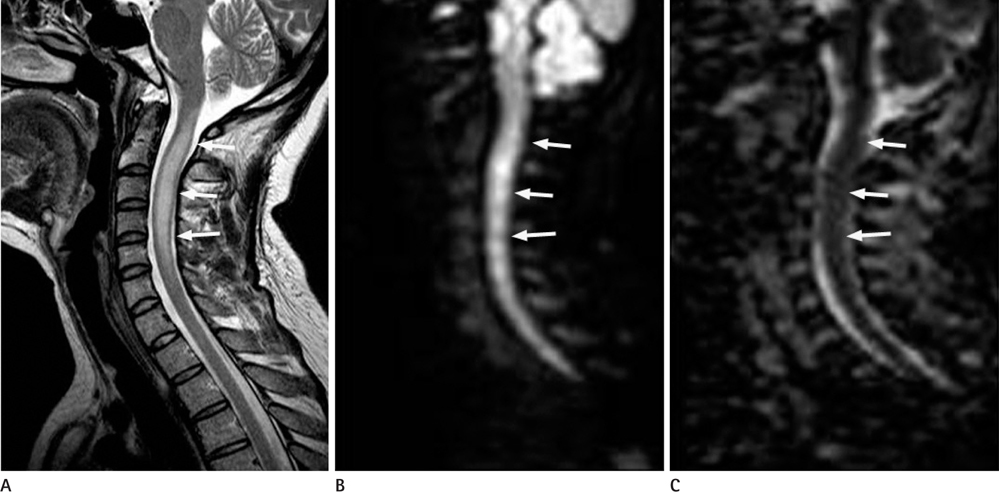
Fig. 1 A 32-year-old woman with acute transverse myelitis. A. Sagittal T2 weighted image shows intramedullary high signal intensity with cord swelling from level C1 to C6 (arrows). B, C. Diffusion weighted image and apparent diffusion coefficient map demonstrate no abnormal signal change (arrows).

Fig. 2 A 49-year-old man with acute transverse myelitis. A. Sagittal T2 weighted image shows intramedullary high signal intensity lesion from level T8 to T11 (arrows). B, C. Diffusion weighted image (B) and apparent diffusion coefficient map (C) illustrate focal diffusion restriction in a cord lesion on a T2 weighted image (arrows).
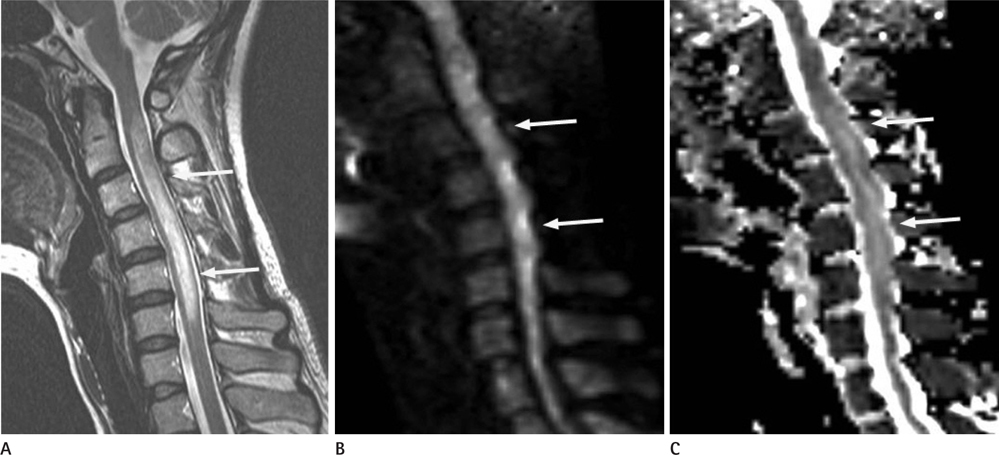
Fig. 3 A 29-year-old woman with acute transverse myelitis. MRI taken 5 days after onset of symptoms. A. Sagittal T2 weighted image shows intramedullary high signal intensity with cord swelling from level C2 to C6 (arrows). B. Diffusion weighted image shows iso-signal intensity, probably due to a summation effect of T2 shine-through effect and increased diffusion (arrows). C. Apparent diffusion coefficient map demonstrates high signal intensity, which implies increased diffusion (arrows).
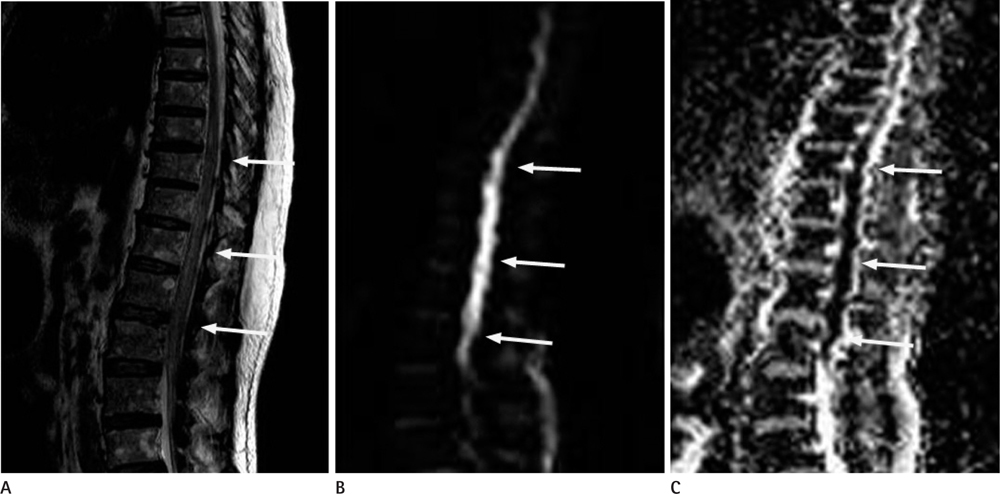
Fig. 4 A 75-year-old woman with a spinal cord infarction. A. Sagittal T2 weighted image illustrates diffuse intramedullary high signal intensity with cord swelling from level T8 to conus (arrows). B, C. Diffusion weighted image and apparent diffusion coefficient map demonstrate diffusion restriction in the affected level (arrows).
Reference
-
1. Holder CA, Muthupillai R, Mukundan S Jr, Eastwood JD, Hudgins PA. Diffusion-weighted MR imaging of the normal human spinal cord in vivo. AJNR Am J Neuroradiol. 2000; 21:1799–1806.2. Bammer R, Fazekas F, Augustin M, Simbrunner J, Strasser-Fuchs S, Seifert T, et al. Diffusion-weighted MR imaging of the spinal cord. AJNR Am J Neuroradiol. 2000; 21:587–591.3. Loher TJ, Bassetti CL, Lövblad KO, Stepper FP, Sturzenegger M, Kiefer C, et al. Diffusion-weighted MRI in acute spinal cord ischaemia. Neuroradiology. 2003; 45:557–561.4. Küker W, Weller M, Klose U, Krapf H, Dichgans J, Nägele T. Diffusion-weighted MRI of spinal cord infarction--high resolution imaging and time course of diffusion abnormality. J Neurol. 2004; 251:818–824.5. Barker GJ. Diffusion-weighted imaging of the spinal cord and optic nerve. J Neurol Sci. 2001; 186:Suppl 1. S45–S49.6. Clark CA, Barker GJ, Tofts PS. Magnetic resonance diffusion imaging of the human cervical spinal cord in vivo. Magn Reson Med. 1999; 41:1269–1273.7. Nedeltchev K, Loher TJ, Stepper F, Arnold M, Schroth G, Mattle HP, et al. Long-term outcome of acute spinal cord ischemia syndrome. Stroke. 2004; 35:560–565.8. Brinar VV, Habek M, Brinar M, Malojcić B, Boban M. The differential diagnosis of acute transverse myelitis. Clin Neurol Neurosurg. 2006; 108:278–283.9. Thurnher MM, Bammer R. Diffusion-weighted MR imaging (DWI) in spinal cord ischemia. Neuroradiology. 2006; 48:795–801.10. Román GC. Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology. 2003; 60:730–731.11. de Seze J, Lanctin C, Lebrun C, Malikova I, Papeix C, Wiertlewski S, et al. Idiopathic acute transverse myelitis: application of the recent diagnostic criteria. Neurology. 2005; 65:1950–1953.12. Jacob A, Weinshenker BG. An approach to the diagnosis of acute transverse myelitis. Semin Neurol. 2008; 28:105–120.13. Krishnan C, Kaplin AI, Deshpande DM, Pardo CA, Kerr DA. Transverse Myelitis: pathogenesis, diagnosis and treatment. Front Biosci. 2004; 9:1483–1499.14. Masson C, Pruvo JP, Meder JF, Cordonnier C, Touzé E, De La Sayette V, et al. Spinal cord infarction: clinical and magnetic resonance imaging findings and short term outcome. J Neurol Neurosurg Psychiatry. 2004; 75:1431–1435.15. Pathak M, Kim RC, Pribram H. Spinal cord infarction following vertebral angiography: clinical and pathological findings. J Spinal Cord Med. 2000; 23:92–95.16. Weidauer S, Nichtweiss M, Lanfermann H, Zanella FE. Spinal cord infarction: MR imaging and clinical features in 16 cases. Neuroradiology. 2002; 44:851–857.17. Lee JW, Park KS, Kim JH, Choi JY, Hong SH, Park SH, et al. Diffusion tensor imaging in idiopathic acute transverse myelitis. AJR Am J Roentgenol. 2008; 191:W52–W57.18. Bhat A, Naguwa S, Cheema G, Gershwin ME. The epidemiology of transverse myelitis. Autoimmun Rev. 2010; 9:A395–A399.19. Kaplin AI, Krishnan C, Deshpande DM, Pardo CA, Kerr DA. Diagnosis and management of acute myelopathies. Neurologist. 2005; 11:2–18.20. Krishnan C, Kaplin AI, Pardo CA, Kerr DA, Keswani SC. Demyelinating disorders: update on transverse myelitis. Curr Neurol Neurosci Rep. 2006; 6:236–243.21. Ramelli GP, Wyttenbach R, von der Weid N, Ozdoba C. Anterior spinal artery syndrome in an adolescent with protein S deficiency. J Child Neurol. 2001; 16:134–135.22. Lewis DW, Packer RJ, Raney B, Rak IW, Belasco J, Lange B. Incidence, presentation, and outcome of spinal cord disease in children with systemic cancer. Pediatrics. 1986; 78:438–443.23. Young G, Krohn KA, Packer RJ. Prothrombin G20210A mutation in a child with spinal cord infarction. J Pediatr. 1999; 134:777–779.24. Beslow LA, Ichord RN, Zimmerman RA, Smith SE, Licht DJ. Role of diffusion MRI in diagnosis of spinal cord infarction in children. Neuropediatrics. 2008; 39:188–191.25. Fujikawa A, Tsuchiya K, Koppera P, Aoki C, Hachiya J. Case report: spinal cord infarction demonstrated on diffusion-weighted MR imaging with a single-shot fast spin-echo sequence. J Comput Assist Tomogr. 2003; 27:415–419.26. Shinoyama M, Takahashi T, Shimizu H, Tominaga T, Suzuki M. Spinal cord infarction demonstrated by diffusion-weighted magnetic resonance imaging. J Clin Neurosci. 2005; 12:466–468.27. Renoux J, Facon D, Fillard P, Huynh I, Lasjaunias P, Ducreux D. MR diffusion tensor imaging and fiber tracking in inflammatory diseases of the spinal cord. AJNR Am J Neuroradiol. 2006; 27:1947–1951.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Spinal Cord Infarction: Diffusion-Weighted MR Imaging: Case Report
- A Rare Case of Syphilitic Myelitis of the Spinal Cord
- A Case of Acute Transverse Myelitis Complicating Diffuse Spinal Cord Atrophy and Syrinx Formation
- Spinal cord stimulation for neuropathic pain following idiopathic transverse myelitis: A case report
- A case of diffuse spinal cord atrophy proven by MRI complicated by acute transverse myelitis
