Coil Embolization of a Ruptured Basilar Tip Aneurysm Associated with Bilateral Cervical Internal Carotid Artery Occlusion: A Case Report and Literature Review
- Affiliations
-
- 1Department of Neurosurgery, Anam Hospital, Korea University Medical Center, Korea University College of Medicine, Seoul, Korea. doctorns@korea.com
- 2Department of Radiology, Anam Hospital, Korea University Medical Center, Korea University College of Medicine, Seoul, Korea.
- 3Department of Neurosurgery, Ansan Hospital, Korea University Medical Center, Korea University College of Medicine, Ansan, Korea.
- KMID: 1441684
- DOI: http://doi.org/10.7461/jcen.2012.14.1.44
Abstract
- We report here on a rare case of a ruptured basilar tip aneurysm that was successfully treated with coil embolization in the bilateral cervical internal carotid artery (ICA) occlusions with abnormal vascular networks from the posterior circulation. A 43-year old man with a familial history of moyamoya disease presented with subarachnoid hemorrhage. Digital subtraction angiography demonstrated complete occlusion of the bilateral ICAs at the proximal portion and a ruptured aneurysm at the basilar artery bifurcation. Each meningeal artery supplied the anterior cranial base, but most of both hemispheres were supplied with blood from the basilar artery and the posterior cerebral arteries through a large number of collateral vessels to the ICA bifurcation as well as the anterior cerebral and middle cerebral arteries. The perfusion computed tomography (CT) scans with acetazolamide (ACZ) injection revealed no reduction of cerebral blood flow and normal cerebrovascular reactivity to ACZ. An abdominal CT aortogram showed no other extracranial vessel abnormalities. A ruptured basilar tip aneurysm was successfully treated with coil embolization without complications. Endovascular embolization may be a good treatment option with excellent safety for a ruptured basilar tip aneurysm that accompanies proximal ICA occlusion with vulnerable collateral flow.
Keyword
MeSH Terms
-
Acetazolamide
Aneurysm
Aneurysm, Ruptured
Angiography, Digital Subtraction
Basilar Artery
Carotid Artery, Internal
Collateral Circulation
Glycosaminoglycans
Meningeal Arteries
Middle Cerebral Artery
Moyamoya Disease
Perfusion
Posterior Cerebral Artery
Skull Base
Subarachnoid Hemorrhage
Acetazolamide
Glycosaminoglycans
Figure
-
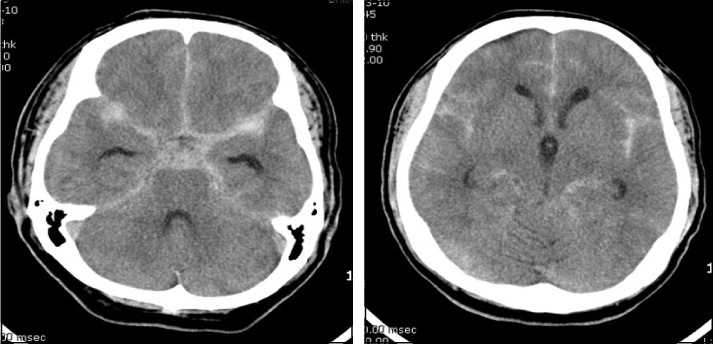
Fig. 1 Brain computed tomography scans demonstrate a diffuse and thick subarachnoid hemorrhage in the bilateral sylvian fissures, the anterior interhemispheric fissure, the basal cistern and the posterior fossa, including the perimesencephalic region.
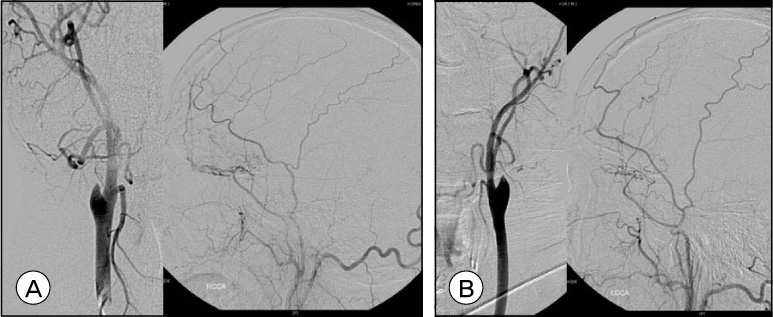
Fig. 2 Right (A) and left (B) carotid digital subtraction angiography scans show complete occlusion of both internal carotid arteries at the level of the carotid bulb without appreciable intracranial filling and small collaterals from both middle meningeal arteries to the anterior cranial fossa.

Fig. 3 A: A vertebral digital subtraction angiography (DSA) demonstrates that both hemispheres are filling in an antegrade fashion from the upper basilar artery and both posterior cerebral arteries through an extensive network of collateral vessels, which mimicked moyamoya vessels, to the internal carotid artery bifurcations. B: A 6 × 4 mm aneurysm is also observed at the basilar artery bifurcation. C: The postembolization DSA shows almost complete obliteration of the aneurysm and patency of the arteries surrounding it.

Fig. 4 Pre-acetazolamide (ACZ) perfusion computed tomography (CT) scans show no abnormalities of the cerebral blood flow (CBF) (A), the cerebral blood volume (CBV) (B) and the mean transit time (MTT) (C). Post-ACZ perfusion CT scans for the CBF (D), CBV (E) and MTT (F) show normal cerebrovascular reactivity to ACZ.
Reference
-
1. AbuRahma AF, Copeland SE. Bilateral internal carotid artery occlusion: natural history and surgical alternatives. Cardiovasc Surg. 1998. 12. 6(6):579–583.
Article2. Adams HP Jr, Kassell NF, Wisoff HS, Drake CG. Intracranial saccular aneurysm and moyamoya disease. Stroke. 1979. 03. 10(2):174–179.
Article3. Arita K, Kurisu K, Ohba S, Shibukawa M, Kiura H, Sakamoto S, et al. Endovascular treatment of basilar tip aneurysms associated with moyamoya disease. Neuroradiology. 2003. 07. 45(7):441–444.
Article4. Irie K, Kawanishi M, Nagao S. Endovascular treatment of basilar tip aneurysm associated with moyamoya disease--case report. Neurol Med Chir (Tokyo). 2000. 10. 40(10):515–518.5. Ishibashi A, Yokokura Y, Kojima K, Abe T. Acute obstructive hydrocephalus due to an unruptured basilar bifurcation aneurysm associated with bilateral internal carotid occlusion--a case report. Kurume Med J. 1993. 40(1):21–25.6. Kagawa K, Ezura M, Shirane R, Takahashi A, Yoshimoto T. Intraaneurysmal embolization of an unruptured basilar tip aneurysm associated with moyamoya disease. J Clin Neurosci. 2001. 09. 8(5):462–464.
Article7. Konishi Y, Sato E, Shiokawa Y, Yazaki H, Hara M, Saito I. A combined surgical and endovascular treatment for a case with five vertebro-basilar aneurysms and bilateral internal carotid artery occlusions. Surg Neurol. 1998. 10. 50(4):363–366.
Article8. Kumagai Y, Sugiyama H, Nawata H, Izeki H, Baba M, Ohta S, et al. [Two cases of pulseless disease with cerebral aneurysm(author's transl)]. No Shinkei Geka. 1981. 04. 9(5):611–615. Japanese.9. Kuroda S, Houkin K. Moyamoya disease: current concepts and future perspectives. Lancet Neurol. 2008. 11. 7(11):1056–1066.
Article10. Massoud TF, Guglielmi G, Vinuela F, Duckwiler GR. Saccular aneurysms in moyamoya disease: endovascular treatment using electrically detachable coils. Surg Neurol. 1994. 06. 41(6):462–467.
Article11. Masuzawa T, Shimabukuro H, Sato F, Furuse M, Fukushima K. The development of intracranial aneurysms associated with pulseless disease. Surg Neurol. 1982. 02. 17(2):132–136.
Article12. Meguro T, Tanabe T, Muraoka K, Terada K, Hirotsune N, Nishino S. Endovascular treatment of aneurysmal subarachnoid hemorrhage associated with bilateral common carotid artery occlusion. Interv Neuroradiol. 2008. 12. 14(4):447–452.
Article13. Muizelaar JP. Early operation of ruptured basilar artery aneurysm associated with bilateral carotid occlusion (moyamoya disease). Clin Neurol Neurosurg. 1988. 06. 90(4):349–355.
Article14. Nagamine Y, Takahashi S, Sonobe M. Multiple intracranial aneurysms associated with moyamoya disease. Case report. J Neurosurg. 1981. 05. 54(5):673–676.15. Shibuya T, Hayashi N. A case of posterior cerebral artery aneurysm associated with idiopathic bilateral internal carotid artery occlusion: case report. Surg Neurol. 1999. 12. 52(6):617–622.
Article16. Suzuki J, Takaku A. Cerebrovascular "moyamoya" disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol. 1969. 03. 20(3):288–299.17. Xu K, Wang H, Luo Q, Li Y, Yu J. Endovascular treatment of bilateral carotid artery occlusion with concurrent basilar apex aneurysm: a case report and literature review. Int J Med Sci. 2011. 03. 8(3):263–269.
Article18. Yamanaka C, Hirohata T, Kiya K, Yoshimoto H, Uozumi T. Basilar bifurcation aneurysm associated with bilateral internal carotid occlusion. Neuroradiology. 1987. 29(1):84–88.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dual Stent-Assisted Coil Embolization for Fusiform Aneurysm Arising From Persistent Trigeminal Artery
- Staged Y-shaped Stent Assisted Coil Embolization in a Wide-Neck Basilar Tip Aneurysm: Case Report
- Stent Assisted Coil Embolization of Unruptured Aneurysm Associated with Basilar Artery Fenestration: A Case Report
- Coil Embolization of Aneurysm Followed by Stereotactic Aspiration of Hematoma in a Patient with Anterior Communicating Artery Aneurysm Presenting with SAH and ICH
- The Efficacy of Simultaneous Bilateral Internal Carotid Angiography during Coil Embolization for Anterior Communicating Artery Aneurysms
