Clinical Analysis of Giant Intracranial Aneurysms with Endovascular Embolization
- Affiliations
-
- 1Department of Neurosurgery, College of medicine, Chosun University, Gwangju, Korea. sjajang@chosun.ac.kr
- KMID: 1441681
- DOI: http://doi.org/10.7461/jcen.2012.14.1.22
Abstract
OBJECTIVE
The purpose of this study was to perform a clinical analysis of nine patients with giant aneurysms managed with endovascular embolization.
METHODS
From March 2000 to September 2009, nine cases of giant intracranial aneurysms were treated (five unruptured and four ruptured). The nine patients included two males and seven females who were 47 to 72 years old (mean, 59.2 years old). The types of giant intracranial aneurysms were eight internal carotid artery aneurysms and one vertebral artery aneurysm. Treatment for each aneurysm was chosen based on anatomic relationships, aneurysmal factors, and the patients' clinical state. Three patients underwent endovascular coiling with stent and six initially underwent endovascular coiling alone. Medical records, operation records, postoperative angiographies, and follow-up angiographies were reviewed retrospectively.
RESULTS
Eight out of nine patients showed good clinical outcomes. (six were excellent and two were good) after a mean follow-up period of 27.9 months. Six (67%) of the nine patients had a near-complete occlusions on the post-operative angiogram (mean, 13.5 months after the procedure). Occlusion rates of 90% or higher were obtained for eight (89%) of all the patients. One patient died due to multiple organ failure. Stents were ultimately required at some point for managing four aneurysms. Two patients needed additional procedures because of aneurysm regrowth.
CONCLUSION
Endovascular treatment could be an alternative option for managing giant aneurysms adjuvant to surgical intervention.
MeSH Terms
Figure
-

Fig. 1 Giant aneurysm on left internal carotid artery (ICA) sized 45 × 31 mm, which compacted coils after 6 months follow-up and then coil compaction was progressed. Another session of coiling was performed. Brain computed tomography (CT) scan without contrast demonstrates an compressive mass (A). Three-dimensional CT angiogram demonstrates a giant aneurysm on left ICA (B). Post-1st Guglielmi detachable coil (GDC) angiogram demonstrates near-complete occlusion of the aneurysm (C). Angiogram demonstrates coil compaction at the neck region at 6 month follow-up (D). Angiogram after additional coiling demonstrates near-complete occlusion of aneurysm (E).
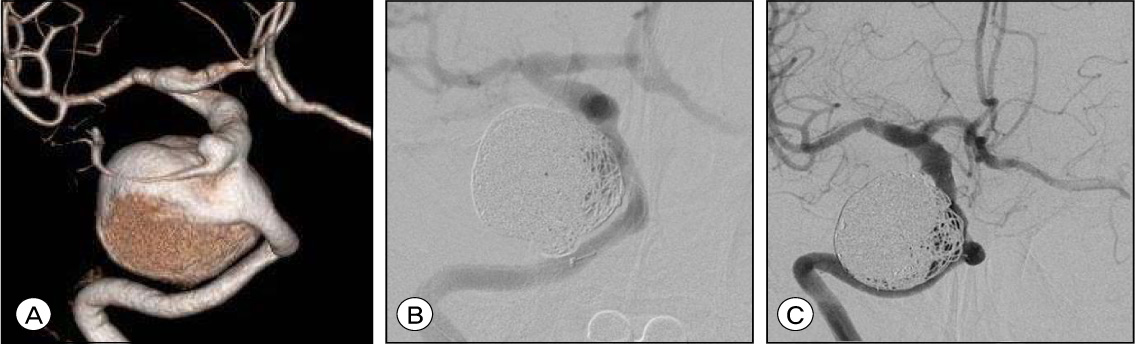
Fig. 2 We performed endovascular coiling on giant aneurysms on right ICA sized 23.4 × 25 mm but small portion of neck is remained unpacked. Three-dimensional CT angiogram demonstrates a giant aneurysm on right ICA (A). Post-GDC angiogram demonstrates small portion of aneurysmal neck unpacked (B and C).

Fig. 3 Giant aneurysm on right ICA sized 25 × 22 mm, which compacted coils and grew again after 12 months follow-up was performed another session of coiling with stent assisting on 24 months after initial session. And then it remained stabilized yet. Three-dimensional CT angiogram demonstrates a giant aneurysm on right ICA (A). Post-GDC (1st) angiogram demonstrates near-complete occlusion of the aneurysm (B). Angiogram demonstrates coil compaction at the neck region at 12 months follow-up (C). Angiogram after 1st additional coiling demonstrates near-complete occlusion of aneurysm (D). Angiogram demonstrates coil compaction at the neck region at 24 months follow-up (E). Angiogram after 2nd additional coiling demonstrates near-complete occlusion of aneurysm (F).
Cited by 1 articles
-
Endosaccular Treatment of Very Large and Giant Intracranial Aneurysms with Parent Artery Preservation : Single Center Experience with Long Term Follow-up
Chae Wook Huh, Jae Il Lee, Chang Hwa Choi, Tae Hong Lee, Jae Young Choi, Jun Kyeung Ko
J Korean Neurosurg Soc. 2018;61(4):450-457. doi: 10.3340/jkns.2017.0606.004.
Reference
-
1. Antunes JL, Correll JW. Cerebral emboli from intracranial aneurysms. Surg Neurol. 1976. 07. 6(1):7–10.2. Arat A, Islak C, Saatci I, Kocer N, Cekirge S. Endovascular parent artery occlusion in large-giant or fusiform distal posterior cerebral artery aneurysms. Neuroradiology. 2002. 08. 44(8):700–705.
Article3. Barrow DL, Alleyne C. Natural history of giant intracranial aneurysms and indications for intervention. Clin Neurosurg. 1995. 42:214–244.4. Battaglia R, Pasqualin A, Da Pian R. Italian cooperative study on giant intracranial aneurysms: 1-Study design and clinical data. Acta Neurochir Suppl (Wien). 1988. 42:49–52.5. Bull J. Massive aneurysms at the base of the brain. Brain. 1969. 92(3):535–570.
Article6. Drake CG. Giant intracranial aneurysms: Experience with surgical treatment in 174 patients. Clin Neurosurg. 1979. 26:12–95.
Article7. Drake CG, Peerless SJ. Giant fusiform intracranial aneurysms: Review of 120 patients treated surgically from. 1965 to 1992. J Neurosurg. 1997. 08. 87(2):141–162.
Article8. Fox AJ, Vinuela F, Pelz DM, Peerless SJ, Ferguson GG, Drake CG, et al. Use of detachable balloons for proximal artery occlusion in the treatment of unclippable cerebral aneurysms. J Neurosurg. 1987. 01. 66(1):40–46.
Article9. Gewirtz RJ, Awad IA. Giant aneurysms of the anterior circle of Willis: Management outcome of open microsurgical treatment. Surg Neurol. 1996. 05. 45(5):409–420. discussion 420-1.
Article10. Gonzalez NR, Duckwiler G, Jahan R, Murayama Y, Vinuela F. Challenges in the endovascular treatment in giant intracranial aneurysms. Neurosurgery. 2006. 11. 59:5 Suppl 3. S113–S124. discussion S3-13.11. Gonzalez N, Murayama Y, Nien YL, Martin N, Frazee J, Duckwiler G, et al. Treatment of unruptured aneurysms with GDCs: Clinical experience with 247 aneurysms. AJNR Am J Neuroradiol. 2004. 04. 25(4):577–583.12. Gruber A, Killer M, Bavinzski G, Richling B. Clinical and angiographic results of endosaccular coiling treatment of giant and very large intracranial aneurysms: A 7-year, single-center experience. Neurosurgery. 1999. 10. 45(4):793–803. discussion 803-4.
Article13. Khanna RK, Malik GM, Qureshi N. Predicting outcome following surgical treatment of unruptured intracranial aneurysms; a proposed grading system. J Neurosurg. 1996. 01. 84(1):49–54.
Article14. Lawton MT, Spetzler RF. Surgical management of giant intracranial aneurysms: Experience with 171 patients. Clin Neurosurg. 1995. 42:245–266.15. Litofsky NS, Vinuela F, Giannotta SL. Progressive visual loss after electrothrombosis treatment of a giant intracranial aneurysm: Case report. Neurosurgery. 1994. 03. 34(3):548–550. discussion 551.16. Pasqualin A, Battaglia R, Scienza R, Da Pian R. Italian cooperative study on giant intracranial aneurysms: 3-Modalities of treatment. Acta Neurochir Suppl (Wien). 1988. 42:60–64.17. Piepgras DG, Khurana VG, Whisnant JP. Ruptured giant intracranial aneurysms: Part II-A retrospective analysis of timing and outcome of surgical treatment. J Neurosurg. 1998. 03. 88(3):430–435.18. Sinson G, Philips MF, Flamm ES. Intraoperative endovascular surgery for cerebral aneurysms. J Neurosurg. 1996. 01. 84(1):63–70.
Article19. Solomon RA, Fink ME, Pile-Spellman J. Surgical management of unruptured intracranial aneurysms. J Neurosurg. 1994. 03. 80(3):440–446.
Article20. Sundt TM. Surgical techniques for saccular and giant intracranial aneurysms. 1990. Baltimore: Williams & Wilkins;7–56.21. Sundt TM Jr, Piepgras DG, Fode NC, Meyer FB. Giant intracranial aneurysms. Clin Neurosurg. 1991. 37:116–154.22. Symon L. Management of giant intracranial aneurysms. Acta Neurochir (Wien). 1992. 116:107–118.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular management of large and giant intracranial aneurysms: Experience from a tertiary care neurosurgery institute in India
- Recent Trends in the Treatment of Cerebral Aneurysms: Comparison between Endovascular Coil Embolization and Surgical Clipping
- Balloon Anchor Technique for Pipeline Embolization Device Deployment Across the Neck of a Giant Intracranial Aneurysm
- Endovascular treatment of intracranial aneurysms: Past and present
- Clinical Experience of Thromboembolic Complications of Coil Embolization for Intracranial Aneurysms with Literature Review
