Hip Pelvis.
2012 Jun;24(2):160-163. 10.5371/hp.2012.24.2.160.
Acute Gluteal Compartment Syndrome without Gluteal Hematoma: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Konyang University, College of Medicine, Daejeon, Korea. ajouos@hanmail.net
- 2Department of Orthopedic Surgery, Ajou University, College of Medicine, Suwon, Korea.
- KMID: 1439106
- DOI: http://doi.org/10.5371/hp.2012.24.2.160
Abstract
- Acute gluteal compartment syndrome (AGCS) is a rare condition associated with trauma, drug abuse, alcohol intoxication, prolonged immobilization, hip arthroplasty and epidural anesthesia. We report the case of a 42-year-old woman presenting severe buttock pain following decreased lower extremity motor function after an incident whereby she rolled down a flight of stairs. We performed fasciotomy of the gluteal fascia in order to provide relief from acute gluteal compartment syndrome. At the 2 month follow up visit her sensory and motor function had improved. Acute gluteal compartment syndrome is a rare condition which can result in misdiagnosis or delayed diagnosis. Careful consideration is needed for patients suffering severe buttock pain.
MeSH Terms
Figure
-

Fig. 1 (A) Preoperative range of motion of ankle dorsiflexion (Grade 0). (B) Preoperative range of motion of great toe dorsiflexion (Grade 0).
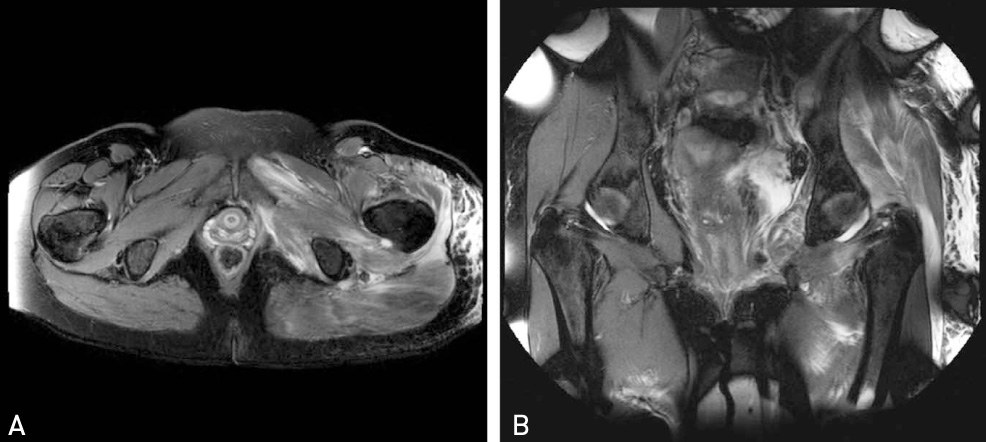
Fig. 2 Preoperative magnetic resonance image of hip; High signal intensity at obturator externus/internus, quadratus femoris, gluteus maximus/medius/minimus, adductor brevis/minimus, pectineus muscles with overlying subcutaneous edema, left.
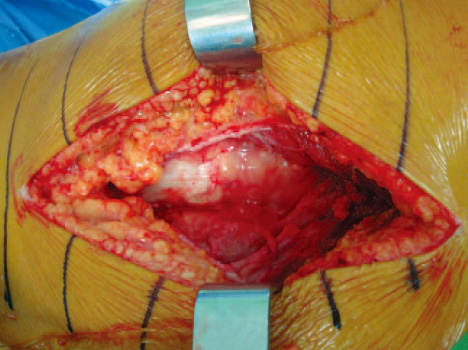
Fig. 3 Intraoperative finding; Subcutaneus edema and fluid collection between iliotibial tract and proximal femur.

Fig. 4 (A) 2 Weeks after Postoperative day; flexion and extension of great toe,ankle was recovered patially (Grade 4), (B) 3 Weeks after Postoperative day; Motor function was nearly full recovered (Grade 4+).
Reference
-
1. Mustafa NM, Hyun A, Kumar JS, Yekkirala L. Gluteal compartment syndrome: a case report. Cases J. 2009. 2:190.
Article2. David V, Thambiah J, Kagda FH, Kumar VP. Bilateral gluteal compartment syndrome. A case report. J Bone Joint Surg Am. 2005. 87:2541–2545.
Article3. Hynes JE, Jackson A. Atraumatic gluteal compartment syndrome. Postgrad Med J. 1994. 70:210–212.
Article4. Somayaji HS, Hassan AN, Reddy K, Heatley FW. Bilateral gluteal compartment syndrome after total hip arthroplasty under epidural anesthesia. J Arthroplasty. 2005. 20:1081–1083.
Article5. Castro-Garcia J, Davis BR, Pirela-Cruz MA. Bilateral gluteal compartment syndrome: a rare but potentially morbid entity. Am Surg. 2010. 76:752–754.
Article6. Keene R, Froelich JM, Milbrandt JC, Idusuyi OB. Bilateral gluteal compartment syndrome following robotic-assisted prostatectomy. Orthopedics. 2010. 33:852.
Article7. Pacheco RJ, Buckley S, Oxborrow NJ, Weeber AC, Allerton K. Gluteal compartment syndrome after total knee arthroplasty with epidural postoperative analgesia. J Bone Joint Surg Br. 2001. 83:739–740.
Article8. Henson JT, Roberts CS, Giannoudis PV. Gluteal compartment syndrome. Acta Orthop Belg. 2009. 75:147–152.9. Liu HL, Wong DS. Gluteal compartment syndrome after prolonged immobilisation. Asian J Surg. 2009. 32:123–126.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Compartment Syndrome of the Gluteus Medius Occurred without Bleeding or Trauma: A Case Report
- Bilateral gluteal compartment syndrome complicated by rhabdomyolysis and acute kidney injury in a patient with alcohol intoxication
- A Case of Hypovolemic Shock Associated with Superior Gluteal Artery Rupture Without Pelvic Fracture in Blunt Trauma
- Gluteal Compartment Syndrome: A Case Report
- Sciatic Nerve Palsy Complicating Gluteal Compartment Syndrome due to Rhabdomyolysis: A Case Report
