Comparison of Floating Knee according to Presence of Knee Joint Injury
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea. osdr2815@naver.com
- 2Department of Orthopedic Surgery, Presbyterian Medical Center, Jeonju, Korea.
- KMID: 1434066
- DOI: http://doi.org/10.12671/jkfs.2012.25.4.277
Abstract
- PURPOSE
To compare the clinical outcomes of floating knee according to the presence of knee joint injury.
MATERIALS AND METHODS
Between March 2004 and March 2009, we investigated 36 patients, who underwent surgical treatment for floating knee injuries. We classified the floating knee into two groups as type I (12 cases) has no knee joint injury and type II (24 cases) has knee joint injury. We compared two groups about combined injury (orthopedics or other part), open fracture or not, neurovascular injury,union time, range of motion, and complication rate.
RESULTS
There is statistically no significant difference between two groups as type I (6 cases, 50%) and type II (13 cases, 54.2%) in orthopedic combined injury (p=0.813), and also same as type I (3 cases, 25%) and type II (12 cases, 50%) in combined injury on the other department (p=0.151), and in floating knee with open fracture as 4 type I (33%) and 12 type II (50%) of 16 cases (44%), and Gustilo-Anderson 3 type I, 4 type II, 1 IIIA, 4 IIIB, and 4 IIIC (p=0.423). There is statistically no significant difference between two groups in neurovascular injury as 1 type I (8.3%), and 3 type II (12.5%) (p=0.708). There is a statistically significant difference between two groups in the mean bone union time as 18.2+/-5.37 weeks (12~24 weeks) for type I and 24.95+/-9.85 weeks (16~33 weeks) for type II (p=0.045), and in the mean range of knee joint motion as 133+/-12.74 degree (120~150 degree) for type I and 105+/-19.00 degree (80~135 degree) for type II (p=0.012).
CONCLUSION
Floating knee with knee joint injury is severe itself and related with severe combined injuries, subsequent range of knee joint motion limitation, the delay of union time, and high complication rate. Therefore, we should take care in surgical treatment for this trauma entity.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Preoperative knee anteroposterior (AP) lateral radiographs show a tibia and femur shaft comminuted fracture, but the fracture line does not extend to the knee joint. (B) Postoperative knee AP lateral radiographs show good reduction with internal fixation device (intramedullary nails). (C) Last follow-up knee AP lateral radiographs show the complete bony healing at fracture sites.
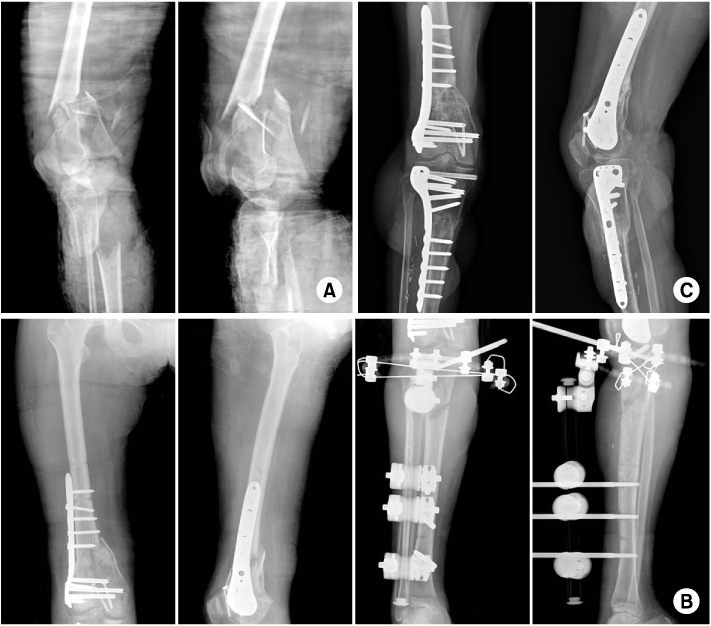
Fig. 2 (A) Preoperative knee antero-posterior (AP) lateral radiographs show femur intra-articular comminuted fracture and tibia open comminuted fracture with posterior tibial artery rupture. (B) Postoperative femur and tibia AP lateral radiographs show plate and screw fixation for the femur and temporary external fixation for the tibia, which was converted to plate and screw fixation after open wound healing. (C) Last follow-up knee AP lateral radiographs show complete bony healing at the fracture sites.
Reference
-
1. Blake R, McBryde A Jr. The floating knee: Ipsilateral fractures of the tibia and femur. South Med J. 1975. 68:13–16.
Article2. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976. 58:453–458.
Article3. Hahn SB, Koh GH. Treatment of Ipsilateral Fracture of the Femur and Tibia("floating knee"). J Korean Soc Fract. 1995. 8:488–496.4. Hayes JT. Multiple fractures in the same extremity: some problems in their management. Surg Clin North Am. 1961. 41:1379–1388.5. Höjer H, Gillquist J, Liljedahl SO. Combined fractures of the femoral and tibial shafts in the same limb. Injury. 1977. 8:206–212.6. Park YB, Moon SH, Hwang CS, Hyun S. Treatment of ipsilateral femur and tibia fractures. J Korean Soc Fract. 1998. 11:754–760.
Article7. Ratliff AHC. Fractures of femur and tibia in the same limb. In Proceedings of the British Orthopaedic Association. J Bone Joint Surg Am. 1975. 47-B:586.
Article8. Rethnam U, Yesupalan RS, Nair R. The floating knee: epidemiology, prognostic indicators & outcome following surgical management. J Trauma Manag Outcomes. 2007. 1:2.
Article9. Veith RG, Winquist RA, Hansen ST Jr. Ipsilateral fractures of the femur and tibia. A report of fifty-seven consecutive cases. J Bone Joint Surg Am. 1984. 66:991–1002.10. Winquist RA. Meyers MH, editor. Segmental fractures of the lower extremity and the floating knee. The multiple injured patient with complex fractures. 1984. Philadelphia: Lea and Febiger;218–248.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Floating Knees Treated by 4 Intramedullary Nails: A Case Report
- Aspiration and Injection of the Knee Joint: Approach Portal
- Irreduccible posterolateral dislocation of the knee joint: a casereport
- The clinical findings of the knee joint tuberoulosis and treatment with synovectomy for preservation of the knee joint motion
- Surgical Treatment of Ipsilateral Fracture of the Femur and Tibia("Floating Knee")
