J Korean Assoc Pediatr Surg.
2012 Dec;18(2):75-82. 10.13029/jkaps.2012.18.2.75.
Significance of Contrast Enema in One-stage Transanal Endorectal Pull-through Operation for Hirschsprung Disease
- Affiliations
-
- 1Department of Pediatric Surgery, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. jtoh@yuhs.ac
- 2Department of Radiology, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1427994
- DOI: http://doi.org/10.13029/jkaps.2012.18.2.75
Abstract
- In one-stage transanal endorectal pull-through operation (TERPT) for Hirschsprung disease, preoperative evaluation by contrast enema (CE) is important tool in aspect of planning of surgical procedure as well as diagnosis. This study was to evaluate the significance of CE for identifying the extent of aganglionic bowel. A retrospective analysis was performed in 40 patients who underwent TERPT between 2003 and 2011. The authors reviewed the CE studies and their correlation with pathologic extent of aganglionosis. Total 66 contrast enemas were performed in 40 patients. Twenty patients underwent single CE, but 20 patients required multiple CEs. In single CE group, 17 had clear radiographic transition zone, but 3 had less definite transition zone. In multiple CE group, 17 patients who had equivocal finding in first or second CE had definite radiographic transition zone, but 3 patients of this group had less definite radiographic transition zones. Overall, 34 patients (85%) had clear radiographic transition zone by single or repeated CE. One (2.9%) out of 34 patients with clear radiographic transition zone had discordance between radiographic and pathologic transition zone. In contrast 4 (66.7%) out of 6 patients with equivocal radiographic transition zone had discordance between radiographic and pathologic transition zone. Observation of clear radiographic transition zone is important in preparation of TERPT, and repeated CE is helpful to reduce the discordance between radiographic and pathologic transition zone. Awareness of the possibility of discordance is also important if radiographic transitional zone is not clear.
Figure
-
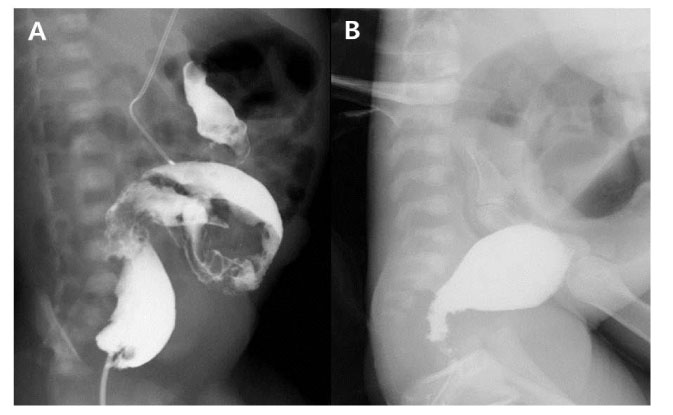
Fig. 1 A case who required repeated contrast enema (CE). Transition zone was not observed in the first CE (A), but clear transition zone was identified in the second CE (B).
Reference
-
1. Swenson O. How the cause and cure of Hirschsprung's disease were discovered. J Pediatr Surg. 1999. 34:1580–1581.2. De la Torre-Mondragón L, Ortega-Salgado JA. Transanal endorectal pull- through for Hirschsprung's disease. J Pediatr Surg. 1998. 33:1283–1286.3. Langer JC, Minkes RK, Mazziotti MV, Skinner MA, Winthrop AL. Transanal one-stage Soave procedure for infants with Hirschsprung's disease. J Pediatr Surg. 1999. 34:148–151. discussion 152.4. Elhalaby EA, Hashish A, Elbarbary MM, Soliman HA, Wishahy MK, Elkholy A, Abdelhay S, Elbehery M, Halawa N, Gobran T, Shehata S, Elkhouly N, Hamza AF. Transanal one-stage endorectal pull-through for Hirschsprung's disease: a multicenter study. J Pediatr Surg. 2004. 39:345–351. discussion 345-351.5. Kim HY, Oh JT. Stabilization period after 1-stage transanal endorectal pull-through operation for Hirschsprung disease. J Pediatr Surg. 2009. 44:1799–1804.6. Langer JC, Seifert M, Minkes RK. One-stage Soave pull-through for Hirschsprung's disease: a comparison of the transanal and open approaches. J Pediatr Surg. 2000. 35:820–822.7. Jamieson DH, Dundas SE, Belushi SA, Cooper M, Blair GK. Does the transition zone reliably delineate aganglionic bowel in Hirschsprung's disease? Pediatric radiology. 2004. 34:811–815.8. O'Donovan AN, Habra G, Somers S, Malone DE, Rees A, Winthrop AL. Diagnosis of Hirschsprung's disease. AJR Am J Roentgenol. 1996. 167:517–520.9. Taxman TL, Yulish BS, Rothstein FC. How useful is the barium enema in the diagnosis of infantile Hirschsprung's disease? Am J Dis Child. 1986. 140:881–884.10. Proctor ML, Traubici J, Langer JC, Gibbs DL, Ein SH, Daneman A, Kim PC. Correlation between radiographic transition zone and level of aganglionosis in Hirschsprung's disease: Implications for surgical approach. J Pediatr Surg. 2003. 38:775–778.11. Aslan MK, Karaman I, Karaman A, Erdogan D, Cavusoglu YH, Cakmak O. Our experience with transanal endorectal pull-through in Hirschsprung's disease. Eur J Pediatr Surg. 2007. 17:335–339.12. El-Sawaf MI, Drongowski RA, Chamberlain JN, Coran AG, Teitelbaum DH. Are the long-term results of the transanal pull-through equal to those of the transabdominal pull-through? A comparison of the 2 approaches for Hirschsprung disease. J Pediatr Surg. 2007. 42:41–47. discussion 47.13. Langer JC, Durrant AC, de la Torre L, Teitelbaum DH, Minkes RK, Caty MG, Wildhaber BE, Ortega SJ, Hirose S, Albanese CT. One-stage transanal Soave pullthrough for Hirschsprung disease: a multicenter experience with 141 children. Ann Surg. 2003. 238:569–583. discussion 583-565.14. Nasr A, Langer JC. Evolution of the technique in the transanal pull-through for Hirschsprung's disease: effect on outcome. J Pediatr Surg. 2007. 42:36–39. discussion 39-40.15. Podevin G, Lardy H, Azzis O, Branchereau S, Petit T, Sfeir R, Weil D, Heloury Y, Fremond B. Technical problems and complications of a transanal pull-through for Hirschsprung's disease. Eur J Pediatr Surg. 2006. 16:104–108.16. Rosenfield NS, Ablow RC, Markowitz RI, DiPietro M, Seashore JH, Touloukian RJ, Cicchetti DV. Hirschsprung disease: accuracy of the barium enema examination. Radiology. 1984. 150:393–400.17. Diamond IR, Casadiego G, Traubici J, Langer JC, Wales PW. The contrast enema for Hirschsprung disease: predictors of a false-positive result. J Pediatr Surg. 2007. 42:792–795.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Laparoscopic-Assisted Endorectal Pull-Through for Hirschsprung's Disease
- Laparoscopic Primary Endorectal Pull-through Procedure (Boley's) for Hirschsprung's Disease
- Short-Term Outcomes of Transanal One-Stage Pull-Through for Hirschsprung's Disease
- Single Stage Transanal Endorectal Pull-through Operation for Hirschsprung’s Disease in Neonate: A Single Center Experience
- Assessment of defecation function beyond infantile period for transanal single-stage endorectal pull-through in Hirschsprung disease
