Progression of Intracranial Hemorrhage after Acute Head Injury
- Affiliations
-
- 1Department of Neurosurgery, Chungbuk National University School of Medicine & Medical Research Institute, Cheongju, Korea. ygk@cbnu.ac.kr
- KMID: 1427359
- DOI: http://doi.org/10.13004/jknts.2009.5.2.62
Abstract
OBJECTIVE
The purpose of this study was to evaluate the risk factors for the development of progressive intracranial hemorrhage (PIH) after acute head injury.
METHODS
175 (one hundred and seventy-five) head trauma patients who visited our hospital and had computerized tomography (CT) scan from January 2005 to December 2006 were investigated. Their medical records, radiological images and readings were analyzed retrospectively.
RESULTS
Of the total 175 patients, 64 (64/175=36.6%) presented PIH. PIH was found in 54 patients (48.6%) of the 111 patient who obtained CT scans within 3 hours after trauma, whereas it was found in 10 (15.7%) of 64 patients who obtained CT more than 3 hours after head trauma. In 64 patients having PIH, the mean time interval between first and second CT scans was 13.8 hours. The risk factors for the development of PIH were cause of trauma, hemorrhagic lesion type, initial Glasow Coma Scale, first CT scan time after trauma.
CONCLUSION
If initial CT scan taken early after trauma shows hemorrhage, continuous supervision of mental status and changes in intracranial pressure, and early follow-up CT scan within 5 to 6 hours is necessary. In addition, because progression of hemorrhage may continue in a patient with hyperacute intracranial hemorrhage who are preparing for surgery, it is recommended to have a CT scan again right before the operation.
MeSH Terms
Figure
-
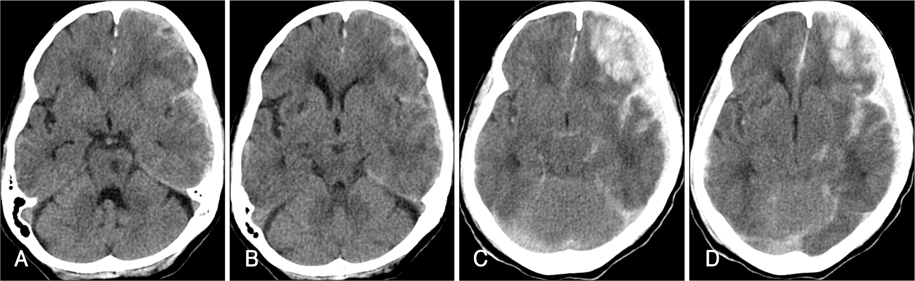
FIGURE 1 Illustration of Case 1, progression of intracranial hemorrhage in 2 hours. A, B: Initial CT scans obtained 30 minutes postinjury, demonstrating multiple small contusion and small amount of subdural hematoma in the left frontotemporal area. C, D: Second CT scans obtained 2 hours postinjury, revealing hemorrhagic progression.
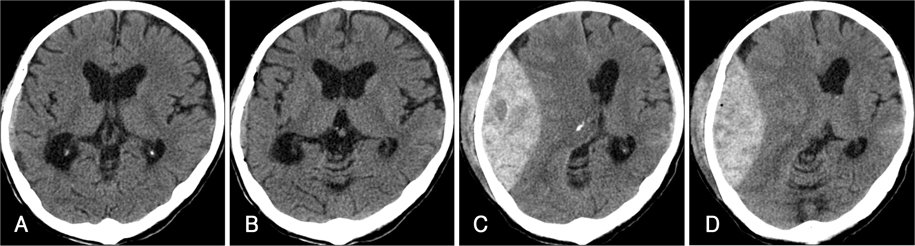
FIGURE 2 Illustration of Case 2, progression of EDH in 5 hours. A, B: Initial CT scans obtained 1 hour postinjury, demonstrating minimal EDH in right temporal lobe. C, D: Second CT scans obtained 6 hours postinjury, revealing large amount of EDH. EDH: epidural hemorrhage.
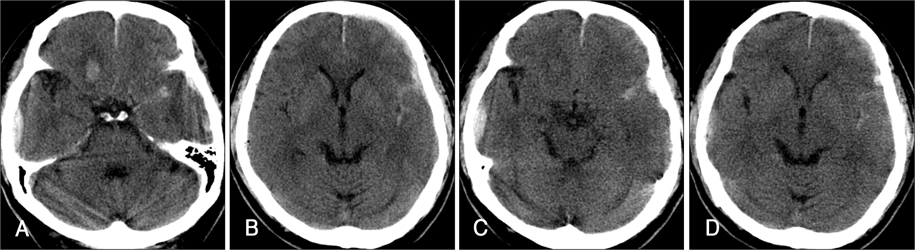
FIGURE 3 Case 3, non progreiion of subdural hemorrhage. A, B: Initial CT scans obtained about 1 day postinjury, demonstrating SDH in the left frontal convexity and multiple contusions. C, D: Second CT scans obtained about 2 days postinjury, revealing no increment of hematoma. SDH: subdural hemorrhage.
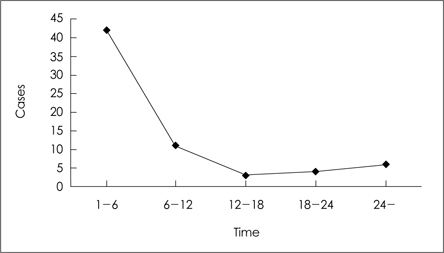
FIGURE 4 Time interval between first and second CT in 64 cases with progressive intracranial hemorrhage.
Cited by 1 articles
-
Risk Factors for Reoperation after Traumatic Intracranial Hemorrhage
Sang-Mi Yang, Sukh Que Park, Sung-Jin Cho, Jae-Chil Chang, Hyung-Ki Park, Ra-Sun Kim
Korean J Neurotrauma. 2013;9(2):114-119. doi: 10.13004/kjnt.2013.9.2.114.
Reference
-
1. Baratham G, Dennyson WG. Delayed traumatic intracerebral hemorrhage. J Neurol Neurosurg Psychiatry. 1972; 35:698–706.2. Becker DP, Miller JD, Ward JD, Greenberg RP, Young HF, Sakalas R. The outcome from severe head injury with early diagnosis and intensive management. J Neurosurg. 1977; 47:491–502.
Article3. Brown CV, Weng J, Oh D, Salim A, Kasotakis G, Demetriades D, et al. Does routine serial computed tomography of the head influence management of traumatic brain injury? A prospective evaluation. J Trauma. 2004; 57:939–943.
Article4. Chang EF, Meeker M, Holland MC. Acute traumatic intraparenchymal hemorrhage: risk factors for progression in the early post-injury period. Neurosurgery. 2006; 58:647–656.
Article5. Clark JA, Finelli RE, Netsky MG. Disseminated intravascular coagulation following cranial trauma. Case report. J Neurosurg. 1980; 52:266–269.6. Crone KR, Lee KS, Kelly DL Jr. Correlation of admission fibrin degradation products with outcome and respiratory failure in patients with severe head injury. Neurosurgery. 1987; 21:532–536.
Article7. Elsner H, Rigamonti D, Corradino G, Schlegel R Jr, Joslyn J. Delayed traumatic intracerebral hematomas: "Spät-Apoplexie". Report of two cases. J Neurosurg. 1990; 72:813–815.8. Gudeman SK, Kishore PR, Miller JD, Girevendulis AK, Lipper MH, Becker DP. The genesis and significance of delayed traumatic intracerebral hematoma. Neurosurgery. 1979; 5:309–313.
Article9. Kaufman HH, Moake JL, Olson JD, Miner ME, duCret RP, Pruessner JL, et al. Delayed and recurrent intracranial hematomas related to disseminated intravascular clotting and fibrinolysis in head injury. Neurosurgery. 1980; 7:445–449.
Article10. Klauber MR, Marshall LF, Toole BM, Knowlton SL, Bowers SA. Cause of decline in head-injury mortality rate in San Diego County, California. J Neurosurg. 1985; 62:528–531.
Article11. Ninchoji T, Uemura K, Shimoyama I, Hinokuma K, Bun T, Nakajima S. Traumatic intracerebral haematomas of delayed onset. Acta Neurochir (Wien). 1984; 71:69–90.
Article12. Oertel M, Kelly DF, McArthur D, Boscardin WJ, Glenn TC, Lee JH, et al. predictors and consequences of the evolving injury. J Neurosurg. 2002; 96:109–116.13. Rathlev NK, Medzon R, Lowery D, Pollack C, Bracken M, Barest G, et al. Intracranial pathology in elders with blunt head trauma. Acad Emerg Med. 2006; 13:302–307.
Article14. Rim BC, Kim ED, Min KS, Lee MS, Kim DH. A clinical analysis of delayed traumatic intracerebral hemorrhage. J Korean Neurosurg Soc. 1998; 27:1490–1499.15. Servadei F, Nanni A, Nasi MT, Zappi D, Vergoni G, Giuliani G, et al. Evolving brain lesions in the first 12 hours after head injury: analysis of 37 comatose patients. Neurosurgery. 1995; 37:899–906.16. Servadei F, Nasi MT, Giuliani G, Cremonini AM, Cenni P, Zappi D, et al. CT prognostic factors in acute subdural haematomas: the value of the 'worst' CT scan. Br J Neurosurg. 2000; 14:110–116.17. Shackford SR, Mackersie RC, Hoyt DB, Baxt WG, Eastman AB, Hammill FN, et al. Impact of a trauma system on outcome of severely injured patients. Arch Surg. 1987; 122:523–527.
Article18. Stein SC, Spettell C, Young G, Ross SE. Delayed and progressive brain injury in closed-head trauma: radiological demonstration. Neurosurgery. 1993; 32:25–30.19. Tabori U, Kornecki A, Sofer S, Constantini S, Paret G, Beck R, et al. Repeat computed tomographic scan within 24-48 hours of admission in children with moderate and severe head trauma. Crit care Med. 2000; 28:840–844.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Oligodendroglioma Presenting as Ventricular Hemorrhage After Head Injury
- Moderate Head Injury: Predictors of a Repeat CT Scan
- Progressive Intracranial Hemorrhage after Acute Head Trauma
- Risk Factors for Reoperation after Traumatic Intracranial Hemorrhage
- Hemorrhagic Complications of Intracranial Arachnoid Cyst Following Minor Head Injury: Report of 5 Cases
