Avascular Necrosis of the Femoral Head in a Patient with Poliomyelitis Treated by THA with a Large-diameter Metal Head - A Case Report -
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Jeonnam, Korea. ospks@jnu.ac.kr
- KMID: 1425039
- DOI: http://doi.org/10.5371/hp.2013.25.1.72
Abstract
- Total hip arthroplasty (THA) can be a good treatment option for avascular necrosis (AVN) of the femoral head. However, because dislocation can frequently occur after surgery, THA is a concern in patients with a neuromuscular disease, such as cerebral palsy or poliomyelitis. In patients with poliomyelitis, only one case of AVN of the femoral head in the affected limb has been reported in the English literature. Here, the authors report on a case of AVN of the femoral head in a patient with poliomyelitis, who was treated with a large diameter femoral head metal-on-metal THA using a modified minimally invasive-2-incision technique.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A, B) Preoperative clinical photograph of the patient walking. He had a left foot deformity, scoliosis with pelvic obliquity, and a Trendelenburg gait.
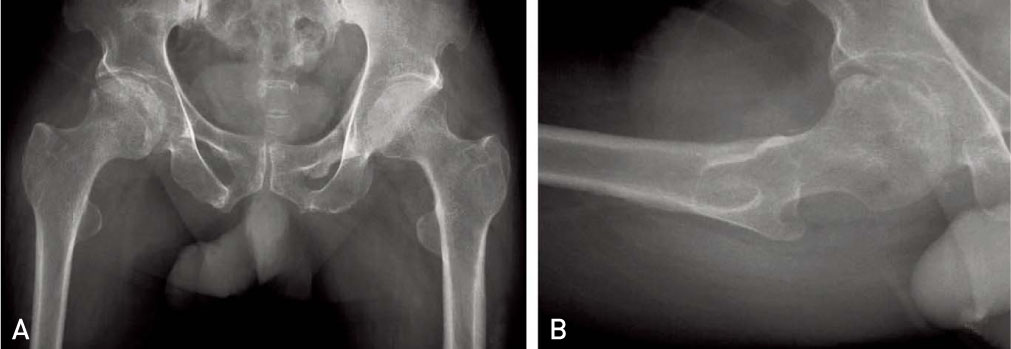
Fig. 2 (A) Preoperative anteroposterior radiograph of both hips showing the crescent sign and sclerotic lesions of the right femoral head. The pelvis was mildly distorted and both proximal femurs were deformed (hip medullary canals were narrow and neck shaft angles were high). (B) Lateral radiograph of the right hip showing the crescent sign on the anterior part of the femoral head.
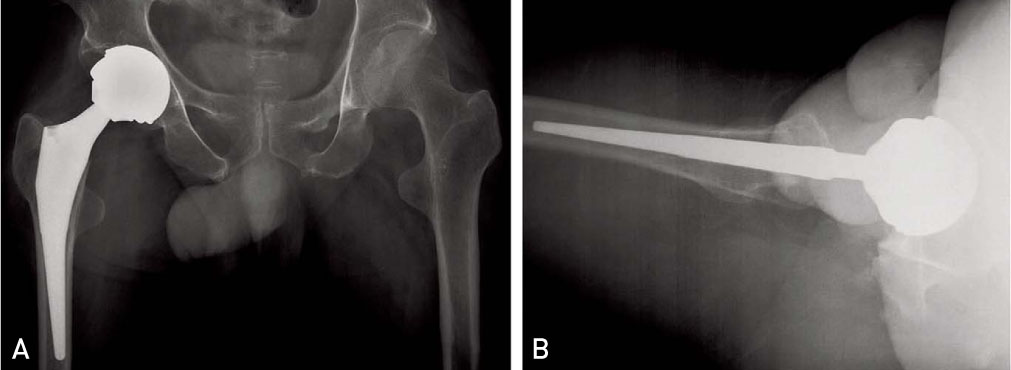
Fig. 3 Plain radiographs taken at two year postoperatively. (A) Both hips anteroposterior and (B) right hip lateral radiographs showing a well bone ingrown acetabular cup and femoral stem. Acetabular abduction and anteversion angles were 57° and 14°, respectively.
Reference
-
1. Cabanela ME, Weber M. Total hip arthroplasty in patients with neuromuscular disease. Instr Course Lect. 2000. 49:163–168.
Article2. Fackler CD, Poss R. Dislocation in total hip arthroplasties. Clin Orthop Relat Res. 1980. (151):169–178.
Article3. Wicart P, Barthas J, Guillaumat M. Replacement arthroplasty of paralytic hip. Apropos of 18 case. Rev Chir Orthop Reparatrice Appar Mot. 1999. 85:581–590.4. Yoon TR, Bae BH, Choi MS. A modified two-incision minimally invasive total hip arthroplasty: technique and short-term results. Hip Int. 2006. 16:Suppl 4. 28–34.
Article5. Yoon TR, Park KS, Song EK, Seon JK, Seo HY. New two-incision minimally invasive total hip arthroplasty: comparison with the one-incision method. J Orthop Sci. 2009. 14:155–160.
Article6. Dabov G, Perez EA. Canale ST, Campbell WC, editors. Miscellaneous nontraumatic disorders. Campbell's operative orthopaedics. 2003. 10th ed. St. Louis, MO: Mosby;957–959.
Article7. Spinnickie A, Goodman SB. Dissociation of the femoral head and trunion after constrained conversion total hip arthroplasty for poliomyelitis. J Arthroplasty. 2007. 22:634–637.
Article8. Kostensalo I, Seppänen M, Mäkelä K, Mokka J, Virolainen P, Hirviniemi J. Early results of large head metal-on-metal hip arthroplasties. Scand J Surg. 2012. 101:62–65.
Article9. Palan J, Beard DJ, Murray DW, Andrew JG, Nolan J. Which approach for total hip arthroplasty: anterolateral or posterior? Clin Orthop Relat Res. 2009. 467:473–477.
Article10. Berry DJ, Berger RA, Callaghan JJ, et al. Minimally invasive total hip arthroplasty Development, early results, and a critical analysis Presented at the Annual Meeting of the American Orthopaedic Association, Charleston, South Carolina, USA, June 14, 2003. J Bone Joint Surg Am. 2003. 85-A:2235–2246.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Femoral Head and Neck Fractures developed in Avascular Necrosis of the Femoral Head
- Bilateral Avascular Necrosis of the Femoral Head in a Patient with Asymptomatic Adrenal Incidentaloma
- Non-traumatic Avascular Necrosis of the Femoral Head
- Histological and Histochemical Study of the Acetabular Articular Cartilage in Avascular Necrosis of Femoral Head
- Increase of Femoral Anteversion after Experimental Induction of Avascular Necrosis of Femoral Head
