Three Dimensional CT-based Virtual Patellar Resection in Female Patients Undergoing Total Knee Replacement: A Comparison between Tendon and Subchondral Method
- Affiliations
-
- 1Division of Arthroplasty, Department of Orthopaedics, Ajou University School of Medicine, Suwon, Korea. thrtkr@ajou.ac.kr
- KMID: 1392981
- DOI: http://doi.org/10.4055/cios.2012.4.3.193
Abstract
- BACKGROUND
Due to its small size, variable shape, and lack of distinct anatomical landmarks, osteoarthritic knees make a precise patellar resection extremely difficult.
METHODS
We performed virtual patellar resection with digital software using three dimensional computed tomography scans of knees from 49 patients who underwent primary total knee replacement at our hospital. We compared 2 commonly used resection methods, the tendon method (TM) and the subchondral method, to determine an ideal resection plane with respect to the symmetry and thickness of the patellar remnant.
RESULTS
The TM gave a thicker resected patella, and a less oval cut surface shape, which gives better coverage for a domed prosthesis. Both methods, however, gave a symmetric resection both superior-inferiorly, as well as mediolaterally.
CONCLUSIONS
Although TM appears statistically better with respect to the thickness and cut surface shape, only further intraoperative studies with long-term clinical follow-up may provide us with the most appropriate patellar resection method.
MeSH Terms
Figure
-

Fig. 1 Reconstruction of three-dimensional (3D) computed tomography images of the knee using specialized computer software. Note the corresponding coronal, sagittal and axial views (2D images) together with the 3D knee image.

Fig. 2 Thickness of the patella on the three-dimensional image is shown by the white arrow.

Fig. 3 Subchondral method showing the plane of resection (white dotted line) in the two-dimensional (2D) axial (A) and 3D sagittal (B) images, and the cut surface in the 2D coronal image (C) showing the cut surface width (W) and height (H) (black line).
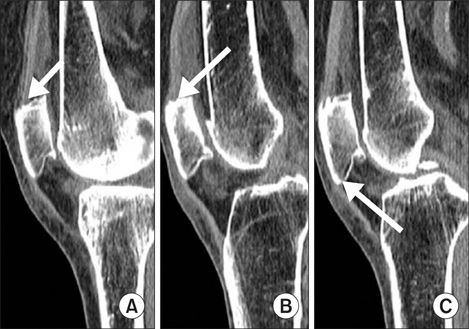
Fig. 4 Anatomic landmarks chosen (white arrows) for resection at the fat fascia-tendon junctions, for the tendon method of resection. Posterior limits of the quadriceps tendon medially (A) and laterally (B) and one at the posterior limit (C) of patellar tendon inferiorly, where the Hounsfield units changed from fat (negative) to fascia-tendon (positive), just outside the bone. These 3 points defined the plane of resection for the tendon method.
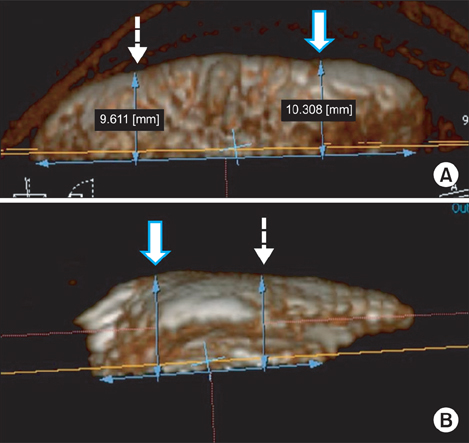
Fig. 5 A-B measurement of the medial (white arrow) and lateral thickness (dotted arrow) for mediolateral symmetry (A) and superior (white arrow) and inferior thickness (dotted arrow) for superoinferior symmetry (B).
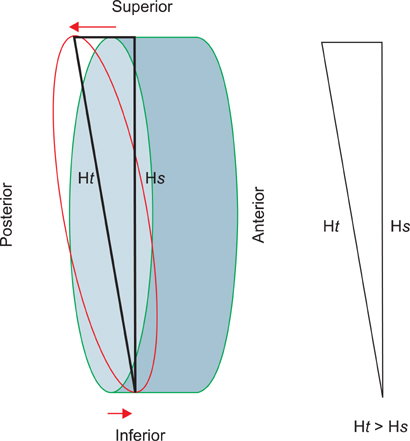
Fig. 6 A schematic representation of the resection planes with the 2 methods. The subchondral method gives a resection surface almost parallel with the anterior surface (green oval), while the tendon method gives a more oblique resection plane (red oval), shown here slightly exaggerated (red arrows). This demonstrates why the cut surface height is more with tendon method (Ht) than with the subchondral method (Hs).
Reference
-
1. Baldini A, Anderson JA, Cerulli-Mariani P, Kalyvas J, Pavlov H, Sculco TP. Patellofemoral evaluation after total knee arthroplasty: validation of a new weight-bearing axial radiographic view. J Bone Joint Surg Am. 2007. 89(8):1810–1817.2. Gomes LS, Bechtold JE, Gustilo RB. Patellar prosthesis positioning in total knee arthroplasty: a roentgenographic study. Clin Orthop Relat Res. 1988. (236):72–81.3. Kim TK, Chung BJ, Kang YG, Chang CB, Seong SC. Clinical implications of anthropometric patellar dimensions for TKA in Asians. Clin Orthop Relat Res. 2009. 467(4):1007–1014.
Article4. Pagnano MW, Trousdale RT. Asymmetric patella resurfacing in total knee arthroplasty. Am J Knee Surg. 2000. 13(4):228–233.5. Baldwin JL, House CK. Anatomic dimensions of the patella measured during total knee arthroplasty. J Arthroplasty. 2005. 20(2):250–257.
Article6. Bengs BC, Scott RD. The effect of patellar thickness on intraoperative knee flexion and patellar tracking in total knee arthroplasty. J Arthroplasty. 2006. 21(5):650–655.
Article7. Hsu HC, Luo ZP, Rand JA, An KN. Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty. 1996. 11(1):69–80.
Article8. Kurosaka M, Yoshiya S, Mizuno K, Yamamoto T. Maximizing flexion after total knee arthroplasty: the need and the pitfalls. J Arthroplasty. 2002. 17:4 Suppl 1. 59–62.
Article9. Anglin C, Fu C, Hodgson AJ, Helmy N, Greidanus NV, Masri BA. Finding and defining the ideal patellar resection plane in total knee arthroplasty. J Biomech. 2009. 42(14):2307–2312.
Article10. Levai JP. Technical aspects: the patellar side. Knee Surg Sports Traumatol Arthrosc. 2001. 9:Suppl 1. S19–S20.
Article11. Ledger M, Shakespeare D, Scaddan M. Accuracy of patellar resection in total knee replacement: a study using the medial pivot knee. Knee. 2005. 12(1):13–19.
Article12. Iranpour F, Merican AM, Amis AA, Cobb JP. The width: thickness ratio of the patella: an aid in knee arthroplasty. Clin Orthop Relat Res. 2008. 466(5):1198–1203.13. Lee TQ, Kim WC. Anatomically based patellar resection criteria for total knee arthroplasty. Am J Knee Surg. 1998. 11(3):161–165.14. Lombardi AV Jr, Mallory TH, Maitino PD, Herrington SM, Kefauver CA. Freehand resection of the patella in total knee arthroplasty referencing the attachments of the quadriceps tendon and patellar tendon. J Arthroplasty. 1998. 13(7):788–792.
Article15. Rand JA. Morrey BF, editor. Total knee arthroplasty: techniques. Joint replacement arthroplasty. 1991. New York, NY: Churchill Livingstone;1002–1003.16. Insall JN. Insall JN, editor. Surgical techniques, instrumentation in total knee arthroplasty. Surgery of the knee. 1993. New York, NY: Churchill Livingstone;767–768.17. Kellgren JH, Lawrence JS. Radiological assessment of osteoarthrosis. Ann Rheum Dis. 1957. 16(4):494–502.
Article18. Healy WL, Wasilewski SA, Takei R, Oberlander M. Patellofemoral complications following total knee arthroplasty: correlation with implant design and patient risk factors. J Arthroplasty. 1995. 10(2):197–201.19. Koh JS, Yeo SJ, Lee BP, Lo NN, Seow KH, Tan SK. Influence of patellar thickness on results of total knee arthroplasty: does a residual bony patellar thickness of <or=12 mm lead to poorer clinical outcome and increased complication rates? J Arthroplasty. 2002. 17(1):56–61.
Article20. Parvizi J, Rapuri VR, Saleh KJ, Kuskowski MA, Sharkey PF, Mont MA. Failure to resurface the patella during total knee arthroplasty may result in more knee pain and secondary surgery. Clin Orthop Relat Res. 2005. 438:191–196.
Article21. Komistek RD, Dennis DA, Mabe JA, Walker SA. An in vivo determination of patellofemoral contact positions. Clin Biomech (Bristol, Avon). 2000. 15(1):29–36.
Article22. Kelly MA. Patellofemoral complications following total knee arthroplasty. Instr Course Lect. 2001. 50:403–407.23. Reuben JD, McDonald CL, Woodard PL, Hennington LJ. Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty. 1991. 6(3):251–258.
Article24. Rauh MA, Bayers-Thering M, Buyea CM, Phillips M, Krackow KA. Reliability and validity of a new caliper for measuring patellar thickness. J Arthroplasty. 2002. 17(1):105–107.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Patellar Tendon Rupture after Total Knee Arthroplasty Revision
- Delayed Repair with Augmentation using Achilles Allograft of Old Ruptured Patellar Tendon after Revison Total Knee Arthroplasty: A Case Report
- Two-stage Reconstruction for Skin and Patellar tendon Defect with Bone-Patellar tendon-Bone Allograft : A Case Report
- Intraarticular Ganglion cyst under Patellar Tendon: Case Report
- Surgical Treatment for Chronic Rupture of the Patellar Tendon Replaced by Fibrotic Scar Tissue
