Subchondral Insufficiency Fractures of the Femoral Head
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kyushu University, Fukuoka, Japan. yamataku@ortho.med.kyushu-u.ac.jp
- KMID: 1392978
- DOI: http://doi.org/10.4055/cios.2012.4.3.173
Abstract
- A subchondral insufficiency fracture (SIF) of the femoral head is a recently proposed concept, which needs to be differentiated from osteonecrosis. Clinically, SIF has generally been observed in the osteoporotic elderly women or renal transplant recipients. Radiographical changes are not obvious in its early phase, however, some cases undergo subchondral collapse (crescent sign). On the T1-weighted magnetic resonance images, a low intensity band is one of the characteristic imaging appearances, which corresponds histologically to the fracture line and associated fracture repair tissue. Therefore, the shape of the low intensity band generally tends to be irregular, disconnected, and convex to the articular surface. The prognosis of SIF is not clearly established. Some cases show resolution of the symptoms by the conservative treatments, while other cases show rapid progression of the collapse such as rapidly progressive arthrosis of the hip.
MeSH Terms
Figure
-
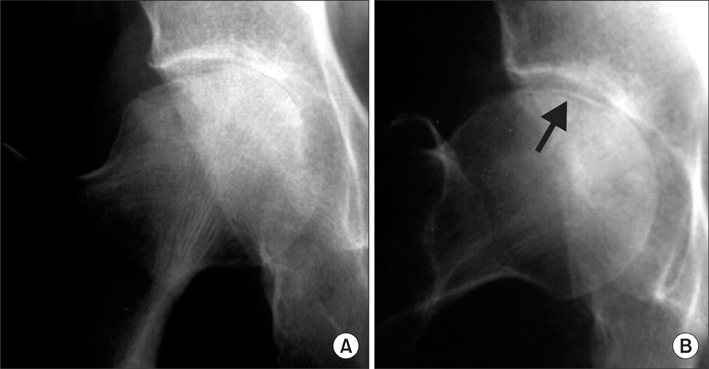
Fig. 1 A 68-year-old woman with a subchondral insufficiency fracture of the right femoral head. (A) Radiograph obtained 8 weeks after onset shows subchondral collapse in the lateral portion of the femoral head. Joint space narrowing is also seen. (B) On the lateral view, a crescent sign is clearly seen (arrow). Final histopathological diagnosis in this case is subchondral insufficiency fracture.
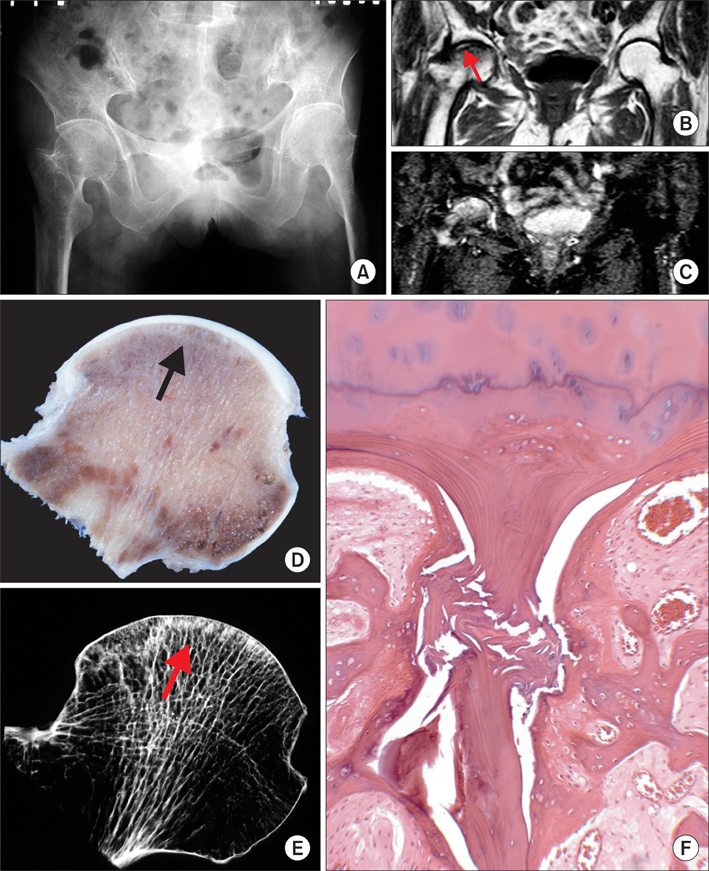
Fig. 2 A 68-year-old woman with a subchondral insufficiency fracture of the right femoral head. (A) Radiograph obtained 4 weeks after onset shows no apparent abnormalities in the femoral head. (B, C) On magnetic resonance imaging obtained 4 weeks after onset, a diffuse bone marrow edema pattern is seen, with low signal intensity on T1-weighted imaging (B) and high signal intensity on T2-weighted imaging (C). A very low signal intensity band parallel to the articular surface is also seen (arrow). (D) On the cut section of the resected femoral head, a whitish line is seen just beneath the articular surface (arrow). (E) The specimen radiograph reveals an osteosclerotic line (arrow), which consists of callus formation along the fracture line (arrow). (F) Histology of the linear sclerotic area shows a fractured original bone trabecula with associated fracture callus formation and granulation tissue in the bone marrow space. No evidence of predisposing osteonecrosis is seen (H&E, ×100). Reprinted from Yamamoto et al.1)
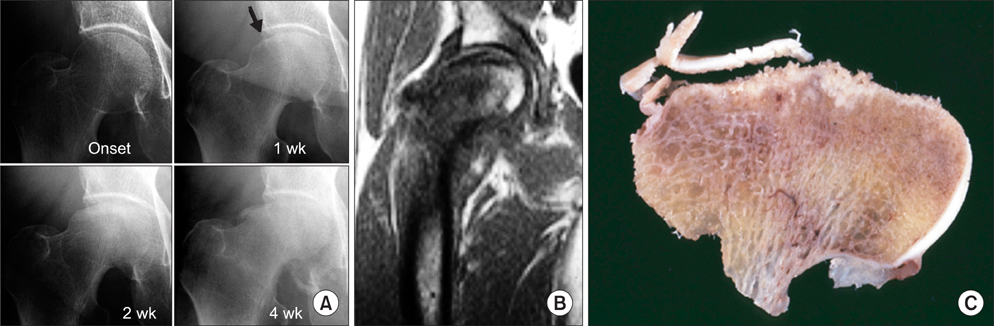
Fig. 3 A 59-year-old woman with a subchondral insufficiency fracture of the right femoral head, which resulted in rapid destruction of the hip joint. (A) No apparent abnormality is seen on the radiograph obtained immediately after the onset of pain. However, a slight collapse was seen on the lateral side of the femoral head 1 week after onset (arrow). The collapse progressed until 4 weeks later, when joint space narrowing, particularly on the medial side, is seen and rapid destruction of the femoral head is observed. (B) Magnetic resonance imaging 2.5 weeks after onset shows a bone marrow edema pattern with two irregularly shaped low intensity bands with a convex shape on T1-weighted imaging. (C) On a cut section of the resected femoral head, a subchondral fracture line is observed with a whitish gray zone consisting of fracture callus and surrounding granulation tissue. The articular cartilage is thin especially in the weight-bearing portion, but its thickness is relatively preserved in the other regions, suggesting no evidence of chondrolysis. Reprinted from Yamamoto et al.16) with permission from American Roentgen Ray Society.
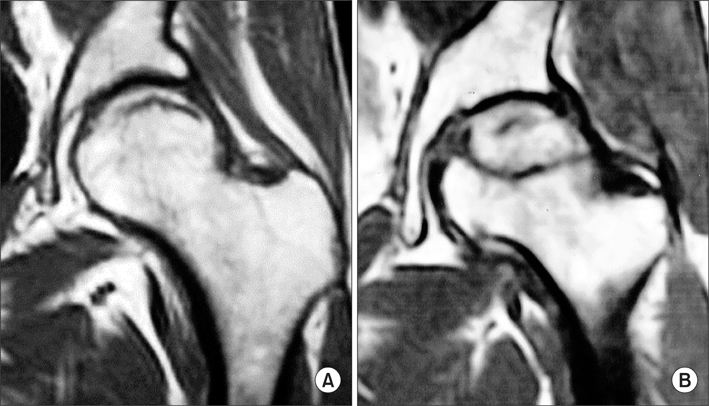
Fig. 4 Comparison of band images in subchondral insufficiency fracture (A) and osteonecrosis (B). Since the band in SIF corresponds to the fracture line, the shape is usually irregular, disconnected, convex and parallel to the cartilage surface. In contrast, the band in osteonecrosis corresponds to repair tissue formed around the necrotic area, which tends to show a smooth, well delineated and concave shape.
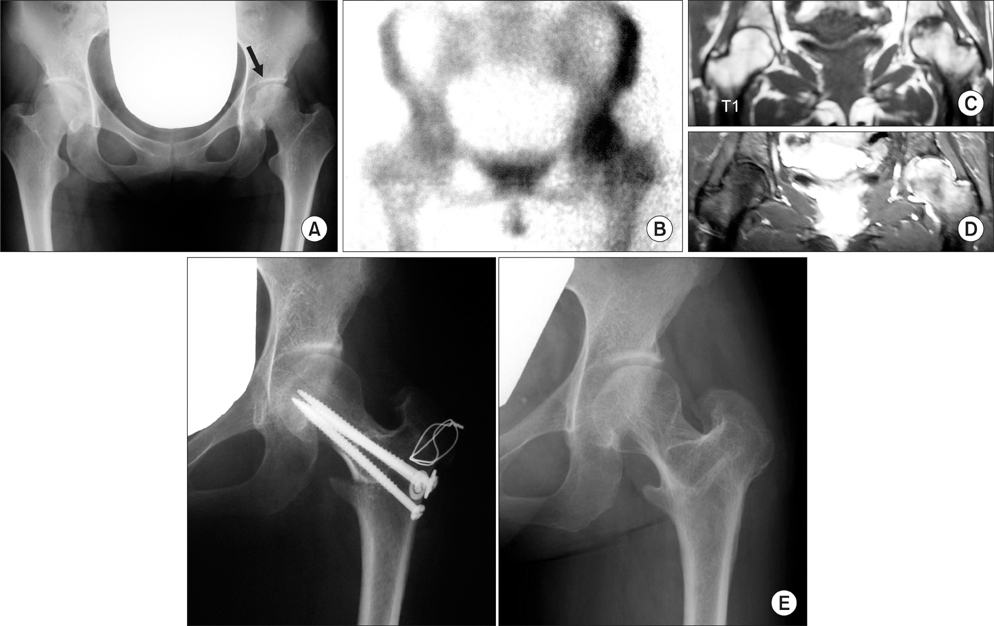
Fig. 5 A 23-year-old woman with a subchondral insufficiency fracture of the left femoral head. (A) Radiograph obtained 2 months after onset shows slight collapse in the lateral portion of the femoral head (arrow) where an irregular joint surface and partial sclerosis are also observed. (B) Bone scintigraphy shows diffuse increased uptake in the femoral head. (C) A low signal intensity area and a band-like pattern are seen on a T1 weighted image. (D) On gadolinium enhanced magnetic resonance imaging, the lesion totally shows diffuse high uptake, indicating that this area is alive. A bone biopsy was performed and the final histopathological diagnosis was subchondral insufficiency fracture in young age. (E) Since fractured lesion is located in the anterosuperior portion, anterior rotational osteotomy was performed to prevent further progression of collapse. Nine years after operation, no evidence of progression of collapse or osteoarthritic change is seen. The patient has no symptom. Partly reprinted from Yamamoto et al.18)

Fig. 6 A 69-year-old man with a subchondral insufficiency fracture of the medial femoral condyle. (A) Radiograph obtained 2 months after onset shows slight collapse of the medial femoral condyle (arrow). A low signal intensity area is seen on T1-weighted image (B) corresponding to high signal intensity on T2-weighted image (C). A bone biopsy was performed and the final histopathological diagnosis was subchondral insufficiency fracture of the medial femoral condyle.
Reference
-
1. Yamamoto T, Iwamoto Y, Schneider R, Bullough PG. Histopathological prevalence of subchondral insufficiency fracture of the femoral head. Ann Rheum Dis. 2008. 67(2):150–153.
Article2. Yamamoto T, Bullough PG. Subchondral insufficiency fracture of the femoral head: a differential diagnosis in acute onset of coxarthrosis in the elderly. Arthritis Rheum. 1999. 42(12):2719–2723.
Article3. Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA. 1964. 187:1001–1004.
Article4. Bangil M, Soubrier M, Dubost JJ, et al. Subchondral insufficiency fracture of the femoral head. Rev Rhum Engl Ed. 1996. 63(11):859–861.5. Cummings SR, Rubin SM, Black D. The future of hip fractures in the United States: numbers, costs, and potential effects of postmenopausal estrogen. Clin Orthop Relat Res. 1990. (252):163–166.6. Visuri T. Stress osteopathy of the femoral head: 10 military recruits followed for 5-11 years. Acta Orthop Scand. 1997. 68(2):138–141.
Article7. Vande Berg BC, Malghem J, Goffin EJ, Duprez TP, Maldague BE. Transient epiphyseal lesions in renal transplant recipients: presumed insufficiency stress fractures. Radiology. 1994. 191(2):403–407.
Article8. Ikemura S, Yamamoto T, Nakashima Y, Shuto T, Jingushi S, Iwamoto Y. Bilateral subchondral insufficiency fracture of the femoral head after renal transplantation: a case report. Arthritis Rheum. 2005. 52(4):1293–1296.
Article9. Iwasaki K, Yamamoto T, Nakashima Y, et al. Subchondral insufficiency fracture of the femoral head after liver transplantation. Skeletal Radiol. 2009. 38(9):925–928.
Article10. Yamamoto T, Schneider R, Iwamoto Y, Bullough PG. Subchondral insufficiency fracture of the femoral head in a patient with systemic lupus erythematosus. Ann Rheum Dis. 2006. 65(6):837–838.
Article11. Yamamoto T, Nakashima Y, Shuto T, Jingushi S, Iwamoto Y. Subchondral insufficiency fracture of the femoral head in younger adults. Skeletal Radiol. 2007. 36:Suppl 1. S38–S42.
Article12. Rafii M, Mitnick H, Klug J, Firooznia H. Insufficiency fracture of the femoral head: MR imaging in three patients. AJR Am J Roentgenol. 1997. 168(1):159–163.
Article13. Yamamoto T, Schneider R, Bullough PG. Subchondral insufficiency fracture of the femoral head: histopathologic correlation with MRI. Skeletal Radiol. 2001. 30(5):247–254.
Article14. Hagino H, Okano T, Teshima R, Nishi T, Yamamoto K. Insufficiency fracture of the femoral head in patients with severe osteoporosis: report of 2 cases. Acta Orthop Scand. 1999. 70(1):87–89.
Article15. Yamamoto T, Bullough PG. The role of subchondral insufficiency fracture in rapid destruction of the hip joint: a preliminary report. Arthritis Rheum. 2000. 43(11):2423–2427.
Article16. Yamamoto T, Takabatake K, Iwamoto Y. Subchondral insufficiency fracture of the femoral head resulting in rapid destruction of the hip joint: a sequential radiographic study. AJR Am J Roentgenol. 2002. 178(2):435–437.
Article17. Iwasaki K, Yamamoto T, Motomura G, et al. Prognostic factors associated with a subchondral insufficiency fracture of the femoral head. Br J Radiol. 2012. 85(1011):214–218.
Article18. Yamamoto T, Iwasaki K, Iwamoto Y. Transtrochanteric rotational osteotomy for a subchondral insufficiency fracture of the femoral head in young adults. Clin Orthop Relat Res. 2010. 468(12):3181–3185.
Article19. Yamamoto T, Schneider R, Bullough PG. Insufficiency subchondral fracture of the femoral head. Am J Surg Pathol. 2000. 24(3):464–468.
Article20. Yamamoto T, DiCarlo EF, Bullough PG. The prevalence and clinicopathological appearance of extension of osteonecrosis in the femoral head. J Bone Joint Surg Br. 1999. 81(2):328–332.
Article21. Yamamoto T, Yamaguchi T, Lee KB, Bullough PG. A clinicopathologic study of osteonecrosis in the osteoarthritic hip. Osteoarthritis Cartilage. 2000. 8(4):303–308.
Article22. Kubo T, Yamazoe S, Sugano N, et al. Initial MRI findings of non-traumatic osteonecrosis of the femoral head in renal allograft recipients. Magn Reson Imaging. 1997. 15(9):1017–1023.
Article23. Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res. 2010. 468(10):2715–2724.
Article24. Ikemura S, Yamamoto T, Motomura G, Nakashima Y, Mawatari T, Iwamoto Y. MRI evaluation of collapsed femoral heads in patients 60 years old or older: differentiation of subchondral insufficiency fracture from osteonecrosis of the femoral head. AJR Am J Roentgenol. 2010. 195(1):W63–W68.
Article25. Zhao G, Yamamoto T, Ikemura S, et al. A histopathological evaluation of a concave-shaped low-intensity band on T1-weighted MR images in a subchondral insufficiency fracture of the femoral head. Skeletal Radiol. 2010. 39(2):185–188.
Article26. Yamaguchi R, Yamamoto T, Motomura G, Ikemura S, Iwamoto Y. MRI-detected double low-intensity bands in osteonecrosis of the femoral head. J Orthop Sci. 2011. 16(4):471–475.
Article27. Mitchell DG, Rao VM, Dalinka MK, et al. Femoral head avascular necrosis: correlation of MR imaging, radiographic staging, radionuclide imaging, and clinical findings. Radiology. 1987. 162(3):709–715.
Article28. Yamamoto T, Bullough PG. Spontaneous osteonecrosis of the knee: the result of subchondral insufficiency fracture. J Bone Joint Surg Am. 2000. 82(6):858–866.
Article29. Tokuya S, Kusumi T, Yamamoto T, Sakurada S, Toh S. Subchondral insufficiency fracture of the humeral head and glenoid resulting in rapidly destructive arthrosis: a case report. J Shoulder Elbow Surg. 2004. 13(1):86–89.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subchondral Stress Fracture of the Femoral Head
- Femoral Head and Neck Fractures developed in Avascular Necrosis of the Femoral Head
- Current Research on Subchondral Insufficiency Fracture of the Femoral Head
- Outcomes of Hybrid Total Hip Arthroplasty for Subchondral Insufficiency Fracture of the Femoral Head
- Repetitive Insufficiency Fractures of the Femoral Shaft: A Case Report
