Fluid Collection in the Right Lateral Portion of the Superior Aortic Recess Mimicking a Right Mediastinal Mass: Assessment with Chest Posterior Anterior and MDCT
- Affiliations
-
- 1Department of Radiology, Gangneung Asan Hospital, College of Medicine, University of Ulsan, Gangneung 210-711, Korea. ryu@gnah.co.kr
- KMID: 1392936
- DOI: http://doi.org/10.3348/kjr.2012.13.5.579
Abstract
OBJECTIVE
We observed patients in whom the fluid collection in the right lateral portion of the superior aortic recess on computed tomography (CT) scans mimicked a right anterior mediastinal mass on chest PA radiographs. The purpose of this study was to assess chest PA and CT features of these patients.
MATERIALS AND METHODS
All chest PA radiographs and CT scans in 9 patients were reviewed by two radiologists on a consensus basis; for the presence of pleural effusion, pulmonary edema and heart size on chest PA radiographs. For the portion of the fluid collection in the superior aortic recess (SAR), a connection between the right lateral portion of the SAR (rSAR) and posterior portion of the SAR (pSAR) on CT scans, and the distance between the right lateral margin of the rSAR and the right lateral margin of the superior vena cava.
RESULTS
Fluid collection in the rSAR on CT scans caused a right anterior mediastinal mass or a bulging contour on chest PA radiographs in all women patients. All patients showed cardiomegaly, five patients had pleural effusion, and two patients had mild pulmonary edema. Further, eight patients showed a connection between the rSAR and the pSAR.
CONCLUSION
The characteristic features of these patients are the right anterior mediastinal mass-like opacity due to fluid collection in the rSAR, are bulging contour with a smooth margin and cardiomegaly regardless of pulmonary edema on the chest PA radiographs, and fluid connection between the rSAR and the pSAR on CT scans.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Aorta, Thoracic/*radiography
Cardiomegaly/radiography
Contrast Media/diagnostic use
Diagnosis, Differential
Female
Humans
Mediastinal Diseases/*radiography
Middle Aged
Pleural Effusion/*radiography
Pulmonary Edema/*radiography
Radiography, Thoracic/*methods
Retrospective Studies
Tomography, X-Ray Computed/*methods
Figure
-

Fig. 1 Normal cross-sectional anatomy of pericardial sinus and recess. A. Cross-sectional drawing of pericardial sinus and recess. B. Due to fluid collection in rSAR, right lateral margin of rSAR migrate into right lateral margin of SVC, wrapping one half of SVC (arrow). rSAR = right lateral portion of superior aortic recess, aSAR = anterior portion of superior aortic recess, pSAR = posterior portion of superior aortic recess, LPR = left pulmonic recess, PPR = posterior pericardial recess, AA = ascending aorta, SVC = superior vena cava, RPA = right pulmonary artery, DA = descending aorta, MPA = main pulmonary artery
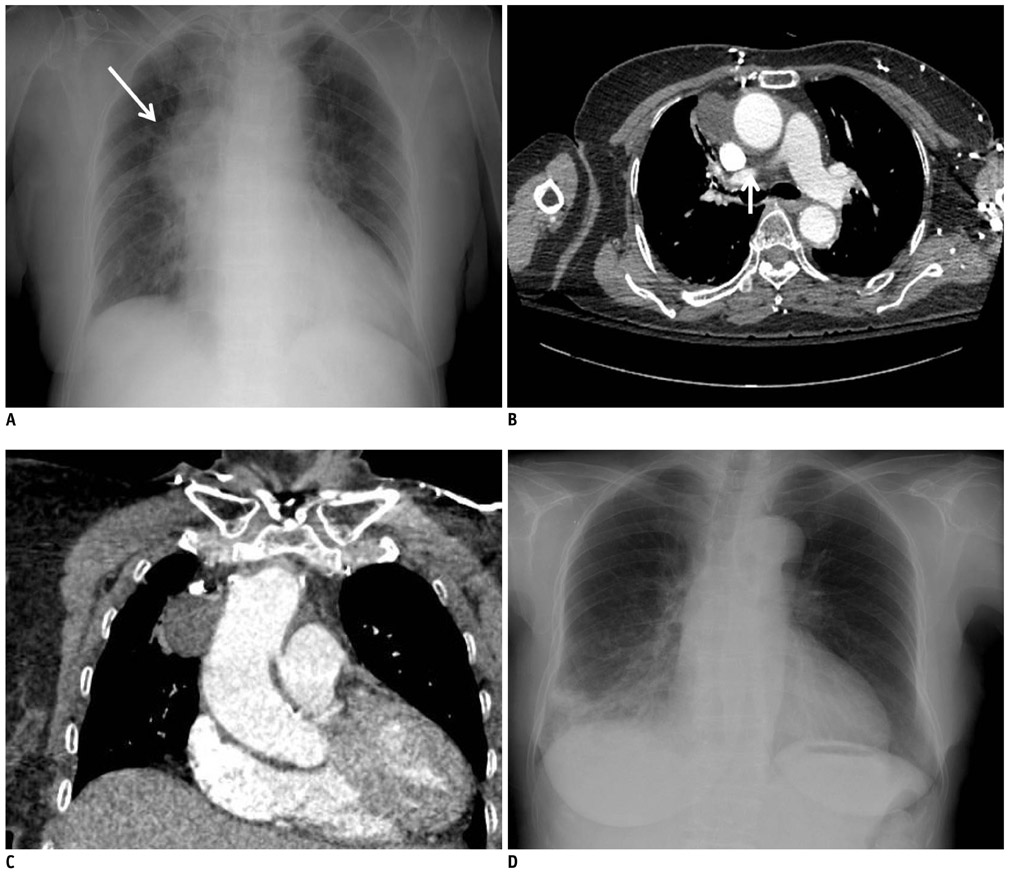
Fig. 2 74 year old female patient with lacunar infarction in right basal ganglia A. Chest PA radiographs shows cardiomegaly without edema and right anterior mediastinal mass (arrow). B. Contrast-enhanced chest CT scans shows moderate amounts of fluid collection in rSAR (long arrow) and connection between rSAR and pSAR (short arrow). C. Multiplanar reconstruction coronal image shows pericardial fluid collection in rSAR, which accounts for convexity on chest PA radiographs. D. Two month follow-up chest PA radiographs shows disappearance of right anterior medastinal mass. PA = posterior-anterior, rSAR = right lateral portion of superior aortic recess, pSAR = posterior portion of superior aortic recess

Fig. 3 81 year old female patient with non ST elevation myocardial infarction. A. Chest PA radiographs shows cardiomegaly with edema and right anterior mediastinal mass (arrow). B. Chest CT shows moderate amounts of fluid collection in rSAR (long arrow) and connection between rSAR and pSAR (short arrow). Small amounts of pleural effusion. C. Two months follow-up chest PA radiograph shows disappearance of right anterior mediastinal mass but cardiomegaly remains. PA = posterior-anterior, rSAR = right lateral portion of superior aortic recess, pSAR = posterior portion of superior aortic recess

Fig. 4 52 year old female patient with T spine fracture. A. Chest PA radiographs shows mild bulging contour (arrow) of right paratracheal area and mild cardiomegaly. B. Chest CT scan at level of great vessel shows low-attenuation lesion (arrow) in right paratracheal region, suggesting high-riding superior pericardial recess. C. Chest CT scan at level of pulmonary artery shows fluid collection in rSAR (arrow). D. Two months follow-up chest PA radiographs shows disappearance of right anterior mediastinal mass. PA = posterior-anterior, rSAR = right lateral portion of superior aortic recess
Reference
-
1. Glazer HS, Siegel MJ, Sagel SS. Low-attenuation mediastinal masses on CT. AJR Am J Roentgenol. 1989. 152:1173–1177.2. Chiles C, Baker ME, Silverman PM. Superior pericardial recess simulating aortic dissection on computed tomography. J Comput Assist Tomogr. 1986. 10:421–423.3. Glazer HS, Aronberg DJ, Sagel SS. Pitfalls in CT recognition of mediastinal lymphadenopathy. AJR Am J Roentgenol. 1985. 144:267–274.4. Moon WK, Im JG, Yeon KM, Han MC. Mediastinal tuberculous lymphadenitis: CT findings of active and inactive disease. AJR Am J Roentgenol. 1998. 170:715–758.5. Kubota H, Sato C, Ohgushi M, Haku T, Sasaki K, Yamaguchi K. Fluid collection in the pericardial sinuses and recesses. Thin-section helical computed tomography observations and hypothesis. Invest Radiol. 1996. 31:603–610.6. Protopapas Z, Westcott JL. Left pulmonic recess of the pericardium: findings at CT and MR imaging. Radiology. 1995. 196:85–88.7. Groell R, Schaffler GJ, Rienmueller R. Pericardial sinuses and recesses: findings at electrocardiographically triggered electron-beam CT. Radiology. 1999. 212:69–73.8. Truong MT, Erasmus JJ, Gladish GW, Sabloff BS, Marom EM, Madewell JE, et al. Anatomy of pericardial recesses on multidetector CT: implications for oncologic imaging. AJR Am J Roentgenol. 2003. 181:1109–1113.9. Kodama F, Fultz PJ, Wandtke JC. Comparing thin-section and thick-section CT of pericardial sinuses and recesses. AJR Am J Roentgenol. 2003. 181:1101–1108.10. Levy-Ravetch M, Auh YH, Rubenstein WA, Whalen JP, Kazam E. CT of the pericardial recesses. AJR Am J Roentgenol. 1985. 144:707–714.11. Aronberg DJ, Peterson RR, Glazer HS, Sagel SS. The superior sinus of the pericardium: CT appearance. Radiology. 1984. 153:489–492.12. Choe YH, Im JG, Park JH, Han MC, Kim CW. The anatomy of the pericardial space: a study in cadavers and patients. AJR Am J Roentgenol. 1987. 149:693–697.13. Winer-Muram HT, Gold RE. Effusion in the superior pericardial recess simulating a mediastinal mass. AJR Am J Roentgenol. 1990. 154:69–71.14. Shin MS, Jolles PR, Ho KJ. CT evaluation of distended pericardial recess presenting as a mediastinal mass. J Comput Assist Tomogr. 1986. 10:860–862.15. Vesely TM, Cahill DR. Cross-sectional anatomy of the pericardial sinuses, recesses, and adjacent structures. Surg Radiol Anat. 1986. 8:221–227.16. Choi YW, McAdams HP, Jeon SC, Seo HS, Hahm CK. The "High-Riding" superior pericardial recess: CT findings. AJR Am J Roentgenol. 2000. 175:1025–1028.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superior Facet Syndrome: Case Report
- A Case of Anterior Mediastinal Mass Presenting with SVC Syndrome
- Radiological Findings of Pleural and Mediastinal Diseases
- Severe hypoxemia and hypotension during general anesthesia of a patient with an anterior mediastinal mass: A case report
- The Changes of the Dimension of Intervertebral Disc,-Neural Foramen and Spinal Canal after Anterior Lumbar Interbody Fusion in the Lumbar Spine
