Aortic Stenosis: Evaluation with Multidetector CT Angiography and MR Imaging
- Affiliations
-
- 1Department of Radiology, Seoul National University Bundang Hospital, Gyeonggi-do, Korea. drsic@radiol.snu.ac.kr
- 2Department of Thoracic Surgery, Seoul National University Bundang Hospital, Gyeonggi-do, Korea.
- 3Department of Internal Medicine, Division of Cardiology, Seoul National University Bundang Hospital, Gyeonggi-do, Korea.
- 4Department of Radiology, Soonchunhyang University Bucheon Hospital, Bucheon, Korea.
- 5Department of Radiology and Institute of Radiation Medicine, Seoul National University College of Medicine, Clinical Research Institute, Seoul National University Hospital, Seoul, Korea.
- KMID: 1385403
- DOI: http://doi.org/10.3348/kjr.2008.9.5.439
Abstract
- Aortic valvular stenosis (AS) is the most common valve disease which results in the need for a valve replacement. Although a Doppler echocardiography is the current reference imaging method, the multidetector computerized tomograpghy (MDCT) and magnetic resonance imaging (MRI) have recently emerged as a promising method for noninvasive valve imaging. In this study, we briefly describe the usefulness and comparative merits of the MDCT and MRI for the evaluation of AS in terms of valvular morphology (as the causes of AS), quantification of aortic valve area, pressure gradient of flow (for assessment severity of AS), and the evaluation of the ascending aorta and cardiac function (as the secondary effects of AS). The familiarity with the MDCT and MRI features of AS is considered to be helpful for the accurate diagnosis and proper management of patients with a poor acoustic window.
MeSH Terms
Figure
-

Fig. 1 Plane selection for evaluation of aortic valve morphology in patient with normal aortic valve on ECG-gated multidetector CT. Note normal three cups and aortic valve in diastolic phase (A, C) and opening in systolic phase (B, D) of double-oblique reconstruction images.
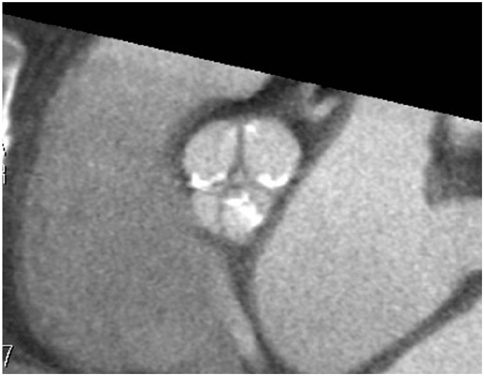
Fig. 2 54-year-old man with severe aortic stenosis. Double-oblique reconstruction image of ECG-gated multidetector CT shows calcified tricuspid valve.

Fig. 3 Incidentally detected non-calcified bicuspid valve that on ECG-gated multidetector CT in systolic phase (A) and diastolic phase (B). Note typical "fishmouth" (arrows) appearance of bicuspid valve in systolic phase.
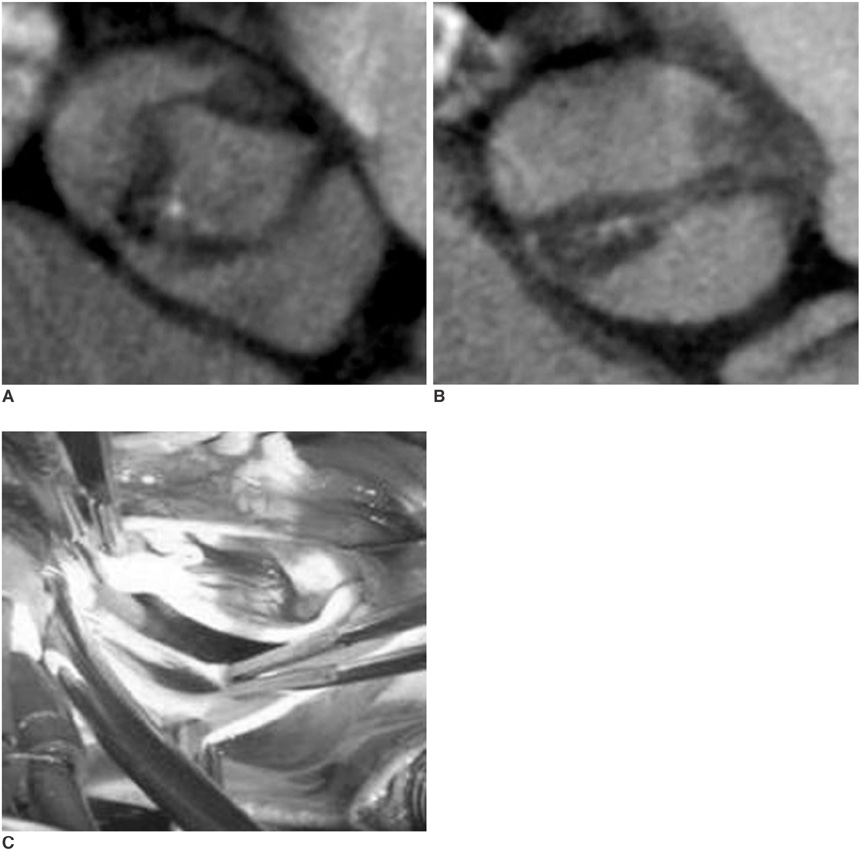
Fig. 4 Thickened bicuspid valve with severe aortic stenosis. Thickened bicuspid valve with severe aortic stenosis from ECG-gated multidetector CT in systolic phase (A) and diastolic phase (B) is well correlated with surgical findings (C).

Fig. 5 Thickened unicommisural unicuspid valve with severe aortic stenosis. Identified thickened unicuspid valve from ECG-gated multidetector CT in systolic phase (A) and diastolic phase (B) is well correlated with surgical findings (C). Note raphe (thin arrows) and calcification (thick arrow) of unicuspid aortic valve.
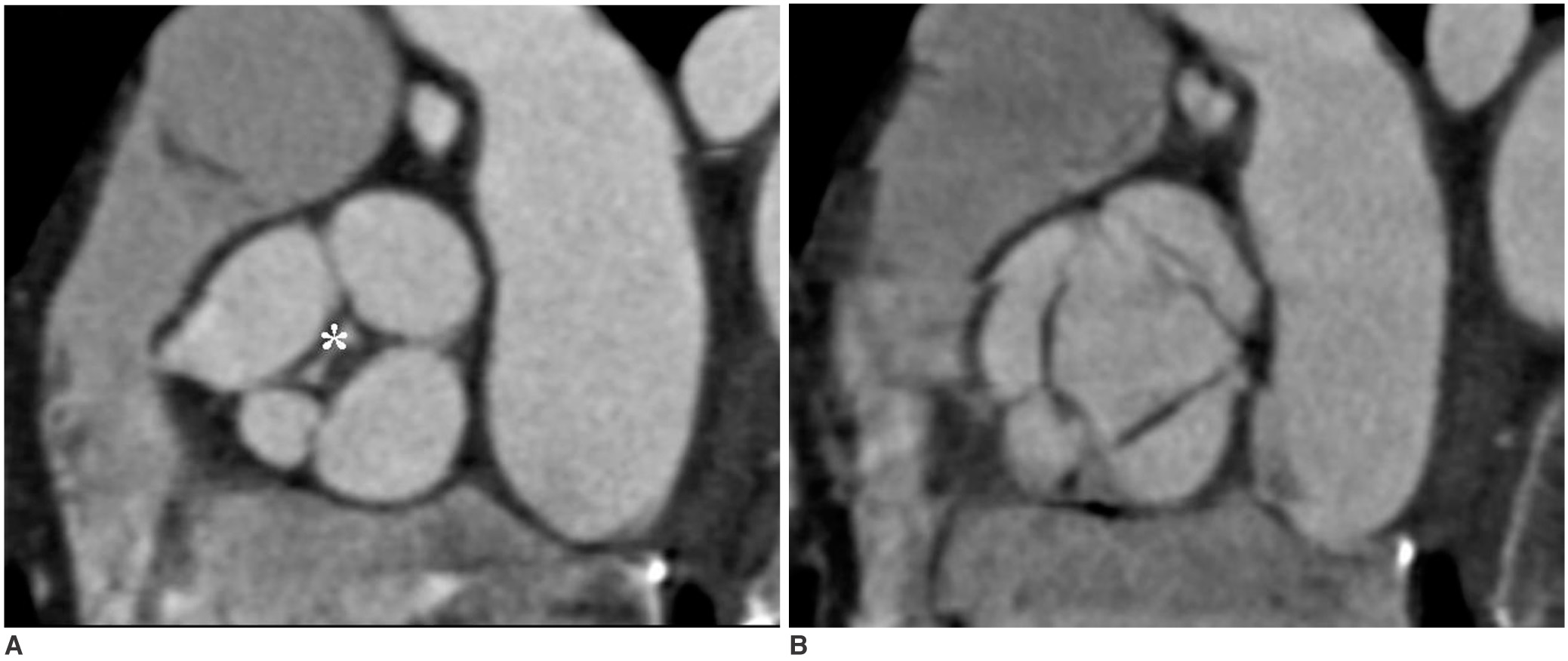
Fig. 6 Multidetector CT scan of aortic valve during diastolic phase (A) and systolic phase (B) shows three equal-sized leaflets and one smaller valve leaflets. Note incomplete coaptation of leaflets centrally (*), resulting in aortic insufficiency.
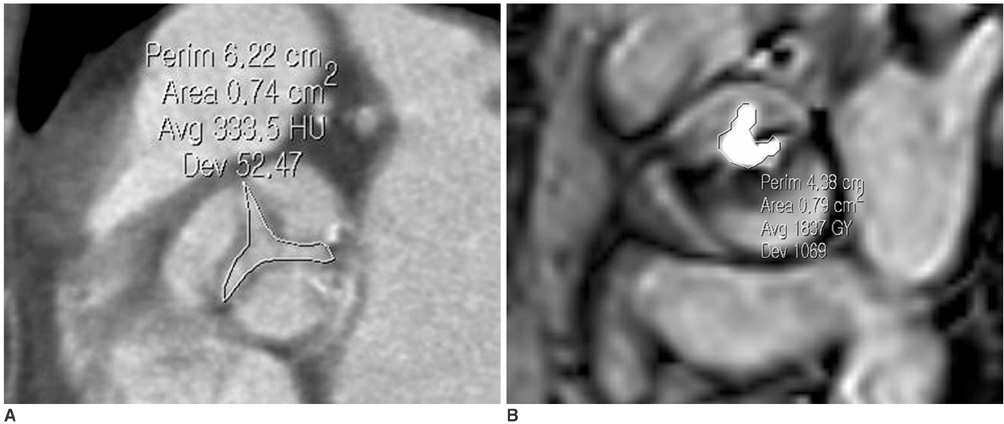
Fig. 7 Measurement of aortic valve area in patients with severe aortic stenosis. Cross-sectional view of severely stenotic tricuspid valve is used for measurement of aortic valve area in systolic phase of ECG-gated multidetector CT image (A) and MRI (B). White line denotes aortic valve area.
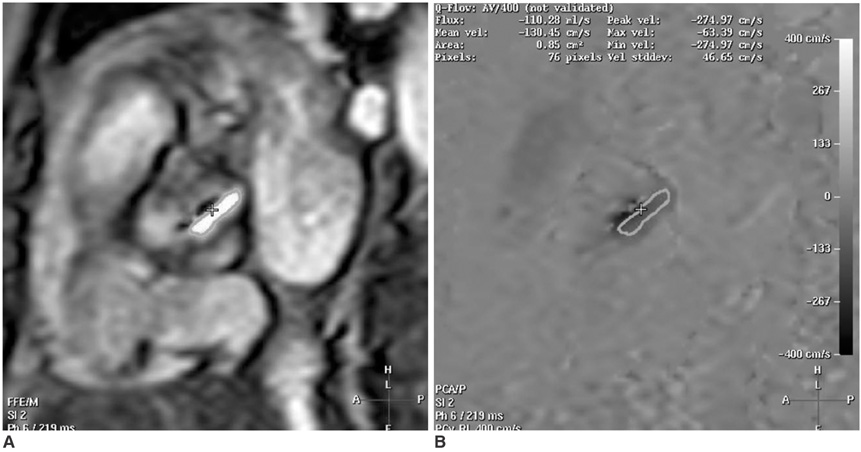
Fig. 8 65-year-old man with severe aortic stenosis and bicuspid aortic valve. Magnitude (A) and phase (B) images for flow measurements of stenotic bicuspid aortic valve using velocity encoded MRI. Line denotes aortic valve area with result of 0.85 cm2. Peak systolic velocity was measured at 547.68 cm/sec, and corresponds to peak pressure gradient of 119 mmHg.

Fig. 9 67-year-old man with severe aortic stenosis. Image of ECG-gated multidetector CT (A) demonstrates post-stenotic dilatation of ascending aorta due to severe aortic stenosis. ECG-gated multidetector CT and MRI can provide accurate sizing of ascending aorta (B).
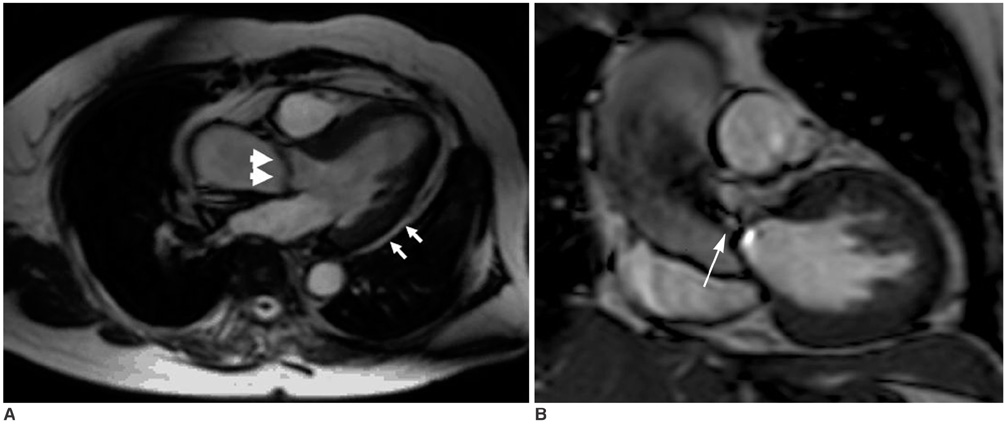
Fig. 10 64-year-old woman with severe aortic stenosis and bicuspid aortic valve. Cine MRI, (A) using steady-state free precession sequence, shows thickened aortic valve (thick small arrows) and left ventricular hypertrophy (small arrows). Flow jet (arrows) is also well visualized (B).
Reference
-
1. Selzer A. Changing aspects of the natural history of valvular aortic stenosis. N Engl J Med. 1987. 317:91–98.2. Dare AJ, Veinot JP, Edwards WD, Tazelaar HD, Schaff HV. New observations on the etiology of aortic valve disease: a surgical pathologic study of 236 cases from 1990. Hum Pathol. 1993. 24:1330–1338.3. Bonow RO, Carabello BA, Kanu C, de Leon AC Jr, Faxon DP, Freed MD, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation. 2006. 114:E84–E231.4. Ryan EW, Bolger AF. Transesophageal echocardiography (TEE) in the evaluation of infective endocarditis. Cardiol Clin. 2000. 18:773–787.5. Bamgartner H. Is there a role for multislice computed tomography in aortic stenosis? Eur Heart J. 2006. 27:2923–2924.6. Pouleur AC, le Polain de Waroux JB, Pasquet A, Vanoverschelde JL, Gerber BL. Aortic valve area assessment: multidetector CT compared with cine MR imaging and transthoracic and transesophageal echocardiography. Radiology. 2007. 244:745–754.7. Lawler LP, Ney D, Pannu HK, Fishman EK. Four-dimensional imaging of the heart based on near-isotropic MDCT data sets. AJR Am J Roentgenol. 2005. 184:774–776.8. Arai AE, Epstein FH, Bove KE, Wolff SD. Visualization of aortic valve leaflets using black blood MRI. J Magn Reson Imaging. 1999. 10:771–777.9. Lotz J, Meier C, Leppert A, Galanski M. Cardiovascular flow measurement with phase-contrast MR imaging: basic facts and implementation. Radiographics. 2002. 22:651–671.10. Jacobs JE, Srichai M, Kim D, Hecht E, Kronzon I. Quadricuspid aortic valve: imaging findings on multidetector helical CT with echocardiographic correlation. J Comput Assist Tomogr. 2006. 30:569–571.11. Alkadhi H, Wildermuth S, Plass A, Bettex D, Baumert B, Leschka S, et al. Aortic stenosis: comparative evaluation of 16-detector row CT and echocardiography. Radiology. 2006. 240:47–55.12. Willmann JK, Weishaupt D, Lachat M, Kobza R, Roos JE, Seifert B, et al. Electrocardiographically gated multi-detector row CT for assessment of valvular morphology and calcification in aortic stenosis. Radiology. 2002. 225:120–128.13. Rosenhek R, Binder T, Porenta G, Lang I, Christ G, Schemper M, et al. Predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med. 2000. 343:611–617.14. Koos R, Mahnken AH, Sinha AM, Wildberger JE, Hoffmann R, Kuhl HP. Aortic valve calcification as a marker for aortic stenosis severity: assessment on 16-MDCT. AJR Am J Roentgenol. 2004. 183:1813–1818.15. Messika-Zeitoun D, Aubry MC, Detaint D, Bielak LF, Peyser PA, Sheedy PF, et al. Evaluation and clinical implications of aortic valve calcification measured by electron-beam computed tomography. Circulation. 2004. 110:356–362.16. Glockner JF, Johnston DL, McGee KP. Evaluation of cardiac valvular disease with MR imaging: qualitative and quantitative techniques. Radiographics. 2003. 23:E9.17. Koos R, Kuhl HP, Muhlenbruch G, Wildberger JE, Gunther RW, Mahnken AH. Prevalence and clinical importance of aortic valve calcification detected incidentally on CT scans: comparison with echocardiography. Radiology. 2006. 241:76–82.18. Liu F, Coursey CA, Grahame-Clarke C, Sciacca RR, Rozenshtein A, Homma S, et al. Aortic valve calcification as an incidental finding at CT of the elderly: severity and location as predictors of aortic stenosis. AJR Am J Roentgenol. 2006. 186:342–349.19. Feuchtner GM, Dichtl W, Friedrich GJ, Frick M, Alber H, Schachner T, et al. Multislice computed tomography for detection of patients with aortic valve stenosis and quantification of severity. J Am Coll Cardiol. 2006. 47:1410–1417.20. Feuchtner GM, Muller S, Bonatti J, Schachner T, Velik-Salchner C, Pachinger O, et al. Sixty-four slice CT evaluation of aortic stenosis using planimetry of the aortic valve area. AJR Am J Roentgenol. 2007. 189:197–203.21. Schlosser T, Malyar N, Jochims M, Breuckmann F, Hunold P, Bruder O, et al. Quantification of aortic valve stenosis in MRI-comparison of steady-state free precession and fast low-angle shot sequences. Eur Radiol. 2007. 17:1284–1290.22. John AS, Dill T, Brandt RR, Rau M, Ricken W, Bachmann G, et al. Magnetic resonance to assess the aortic valve area in aortic stenosis: how does it compare to current diagnostic standards? J Am Coll Cardiol. 2003. 42:519–526.23. Caruthers SD, Lin SJ, Brown P, Watkins MP, Williams TA, Lehr KA, et al. Practical value of cardiac magnetic resonance for clinical quantification of aortic valve stenosis: comparison with echocardiography. Circulation. 2003. 108:2236–2243.24. Eichenberger AC, Jenni R, von Schulthess GK. Aortic valve pressure gradients in patients with aortic valve stenosis: quantification with velocity-encoded cine MR imaging. AJR Am J Roentgenol. 1993. 160:971–977.25. Sondergaard L, Stahlberg F, Thomsen C. Magnetic resonance imaging of valvular heart disease. J Magn Reson Imaging. 1999. 10:627–638.26. Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU, et al. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002. 90:29–34.27. van der Vleuten PA, Willems TP, Götte MJ, Tio RA, Greuter MJ, Zijlstra F, et al. Quantification of global left ventricular function: comparison of multidetector computed tomography and magnetic resonance imaging. A meta-analysis and review of the current literature. Acta Radiol. 2006. 47:1049–1057.28. Yamamuro M, Tadamura E, Kubo S, Toyoda H, Nishina T, Ohba M, et al. Cardiac functional analysis by multi-detector row CT and segmental reconstruction algorithm: comparison with echocardiography, SPECT and MR imaging. Radiology. 2005. 234:381–390.29. Bamgartner H. Is there a role for multislice computed tomography in aortic stenosis? Eur Heart J. 2006. 27:2923–2924.30. Gilard M, Cornily JC, Pennec PY, Joret C, Le Gal G, Mansourati J, et al. Accuracy of multislice computed tomography in the preoperative assessment of coronary disease in patients with aortic valve stenosis. J Am Coll Cardiol. 2006. 47:2020–2024.
