Vascular Complications of Pancreatitis: Role of Interventional Therapy
- Affiliations
-
- 1Diagnostic and Interventional Radiology at University of Texas Health Science Center at San Antonio, San Antonio, Tx 78249, USA. BARGE@UTHSCSA.EDU
- 2Vascular and Interventional Radiology at University of Texas Health Science Center at San Antonio, San Antonio, Tx 78249, USA.
- KMID: 1372867
- DOI: http://doi.org/10.3348/kjr.2012.13.S1.S45
Abstract
- Major vascular complications related to pancreatitis can cause life-threatening hemorrhage and have to be dealt with as an emergency, utilizing a multidisciplinary approach of angiography, endoscopy or surgery. These may occur secondary to direct vascular injuries, which result in the formation of splanchnic pseudoaneurysms, gastrointestinal etiologies such as peptic ulcer disease and gastroesophageal varices, and post-operative bleeding related to pancreatic surgery. In this review article, we discuss the pathophysiologic mechanisms, diagnostic modalities, and treatment of pancreatic vascular complications, with a focus on the role of minimally-invasive interventional therapies such as angioembolization, endovascular stenting, and ultrasound-guided percutaneous thrombin injection in their management.
MeSH Terms
-
Diagnostic Imaging
Embolization, Therapeutic/methods
Hemostasis, Endoscopic
Hemostatics/administration & dosage
Humans
Pancreatitis/*complications
Stents
Thrombin/administration & dosage
Ultrasonography, Interventional
Vascular Diseases/diagnosis/*etiology/physiopathology/*therapy
Vascular Surgical Procedures/*methods
Figure
-

Fig. 1 82-year-old patient with history of common bile duct stent placement and prior gastroduodenal coil embolization presents with severe pancreatitis and blood loss. A. Axial CT image demonstrates walled-off pancreatic necrosis (arrowhead) and new peripancreatic pseudoaneurysm arising from splenic artery (arrow). B. Angiogram confirms active contrast extravasation from splenic artery (arrow). C. Coils are deployed in mid-portion of splenic artery (arrow) distal and proximal to site of contrast extravasation ("sandwich" technique). Also seen is common trunk of superior mesenteric artery and celiac axis (arrowhead). D. Follow-up axial CT image demonstrates interval splenic infarction and development of splenic abscess (arrow); complication related to embolization. Patient ultimately died from multi-organ failure.

Fig. 2 Patient with severe blood loss after Whipple procedure. A, B. 3D reconstructed CT image and angiogram demonstrate large pseudoaneurysm arising from mid-common hepatic artery (arrows). This is inexpendable artery and coil embolization of artery is contraindicated due to possibility of end-organ ischemia. C. Thus, covered stent-graft was deployed across site of arterial injury with complete exclusion of pseudoaneurysm. Another strategy would have been to coil embolize pseudoaneurysm directly if stent-graft deployment was not feasible. (Case courtesy of Dr. Bart Dolmatch, University of Texas Southwestern, Dallas, TX, USA).

Fig. 3 32-year-old patient with chronic pancreatitis who had previously undergone splenectomy for splenic vein thrombosis presents with abdominal pain and blood loss. A. Axial CT image, one year prior, demonstrates moderate-sized pseudocyst in the region of pancreatic body (arrow). B. Axial CT image, one year later, shows interval conversion of this long-standing pseudocyst into pseudoaneurysm (arrow). C. Left gastric arteriogram reveals large pseudoaneurysm arising from proximal aspect of inferior branch (arrow). D. Using microcatheter, coil embolization is performed distal and proximal to arterial injury ("sandwich" technique) (arrowheads).

Fig. 4 Patient with chronic pancreatitis who presents with abdominal pain and blood loss. A. Axial CT angiography image reveals large hemorrhagic pseudocyst adjacent to pancreatic head (arrow) with mass effect causing biliary dilation. Active contrast extravasation is seen anteriorly (arrowhead). Another large pseudocyst is also present in right posterior pararenal space causing mass effect upon right kidney. B. Celiac angiogram confirms contrast extravasation from gastroduodenal artery (GDA) (arrow). C. A microcatheter is advanced distal to arterial injury in GDA and coil embolization performed distal to proximal (arrowheads). D. Follow-up targeted ultrasound confirms thrombosis of pseudoaneurysm.

Fig. 5 Patient with history of pancreatitis who presents with blood loss. A. Angiogram demonstrates distal splenic arterial pseudoaneurysm (arrow). B. Pseudoaneurysm was coil embolized using microcatheter with complete exclusion (arrowheads). C. However, patient continued to bleed during his admission and repeat catheter angiography discovered additional small pseudoaneurysm arising from branch of distal pancreatic artery (arrow). D. Using microcatheter technique, single coil was deployed in this arterial branch proximal to pseudoaneurysm with adequate exclusion (arrowhead).
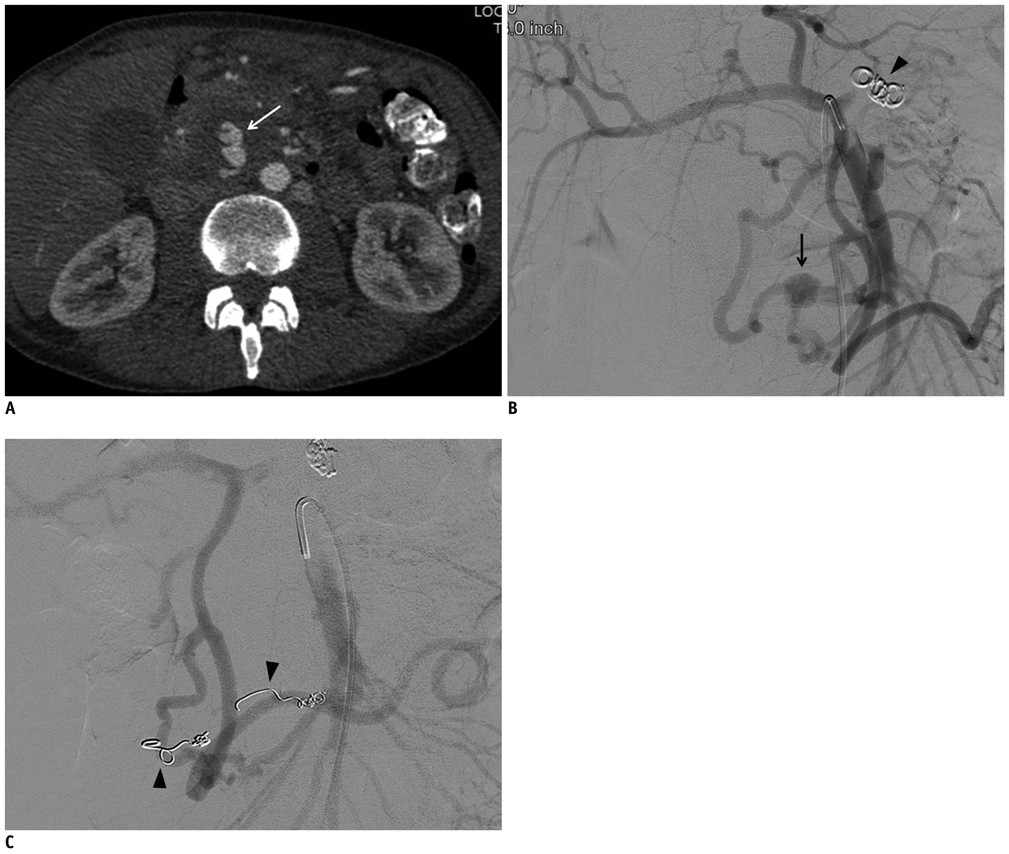
Fig. 6 46-year-old patient with history of chronic pancreatitis and prior splenic embolization, who presented with abdominal pain and blood loss. A. Axial CT angiography image demonstrates bilobed pseudoaneurysm arising from inferior pancreaticoduodenal arcade near pancreatic head (arrow). B. Superior mesenteric artery angiogram confirms presence of pseudoaneurysm arising from branch of inferior pancreaticoduodenal arcade (arrow). Prior splenic embolization coils are also seen (arrowhead). C. Coil embolization is performed of this branch distal and proximal to arterial injury (arrowheads) using microcatheter technique with complete exclusion of pseudoaneurysm. Collateral circulation supplies superior pancreaticoduodenal, gastroduodenal, and proper hepatic arteries.
Reference
-
1. Affronti J. Chronic pancreatitis and exocrine insufficiency. Prim Care. 2011. 38:515–537. ix2. Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006. 354:2142–2150.3. Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology. 2002. 223:603–613.4. Flati G, Andrén-Sandberg A, La Pinta M, Porowska B, Carboni M. Potentially fatal bleeding in acute pancreatitis: pathophysiology, prevention, and treatment. Pancreas. 2003. 26:8–14.5. Sharma PK, Madan K, Garg PK. Hemorrhage in acute pancreatitis: should gastrointestinal bleeding be considered an organ failure? Pancreas. 2008. 36:141–145.6. Bergert H, Dobrowolski F, Caffier S, Bloomenthal A, Hinterseher I, Saeger HD. Prevalence and treatment of bleeding complications in chronic pancreatitis. Langenbecks Arch Surg. 2004. 389:504–510.7. Yekebas EF, Wolfram L, Cataldegirmen G, Habermann CR, Bogoevski D, Koenig AM, et al. Postpancreatectomy hemorrhage: diagnosis and treatment: an analysis in 1669 consecutive pancreatic resections. Ann Surg. 2007. 246:269–280.8. Izaki K, Yamaguchi M, Kawasaki R, Okada T, Sugimura K, Sugimoto K. N-butyl cyanoacrylate embolization for pseudoaneurysms complicating pancreatitis or pancreatectomy. J Vasc Interv Radiol. 2011. 22:302–308.9. Andersson E, Ansari D, Andersson R. Major haemorrhagic complications of acute pancreatitis. Br J Surg. 2010. 97:1379–1384.10. Iwama Y, Sugimoto K, Zamora CA, Yamaguchi M, Tsurusaki M, Taniguchi T, et al. Transcatheter embolization of splenic artery pseudo-aneurysm rupturing into colon after post-operative pancreatitis. Cardiovasc Intervent Radiol. 2006. 29:133–136.11. Charvat F, Maskova J, Belina F, Buric I, Lacman J, Fuksa Z, et al. Portal vein erosion: a rare hemorrhagic complication of acute pancreatitis treated by percutaneous stent-graft placement. J Vasc Interv Radiol. 2010. 21:411–412.12. Lee KM, Paik CN, Chung WC, Yang JM. Association between acute pancreatitis and peptic ulcer disease. World J Gastroenterol. 2011. 17:1058–1062.13. Saad NE, Saad WE, Davies MG, Waldman DL, Fultz PJ, Rubens DJ. Pseudoaneurysms and the role of minimally invasive techniques in their management. Radiographics. 2005. 25:Suppl 1. S173–S189.14. Balachandra S, Siriwardena AK. Systematic appraisal of the management of the major vascular complications of pancreatitis. Am J Surg. 2005. 190:489–495.15. Hsu JT, Yeh CN, Hung CF, Chen HM, Hwang TL, Jan YY, et al. Management and outcome of bleeding pseudoaneurysm associated with chronic pancreatitis. BMC Gastroenterol. 2006. 6:3.16. Harvey J, Dardik H, Impeduglia T, Woo D, DeBernardis F. Endovascular management of hepatic artery pseudoaneurysm hemorrhage complicating pancreaticoduodenectomy. J Vasc Surg. 2006. 43:613–617.17. Zyromski NJ, Vieira C, Stecker M, Nakeeb A, Pitt HA, Lillemoe KD, et al. Improved outcomes in postoperative and pancreatitis-related visceral pseudoaneurysms. J Gastrointest Surg. 2007. 11:50–55.18. Udd M, Leppäniemi AK, Bidel S, Keto P, Roth WD, Haapiainen RK. Treatment of bleeding pseudoaneurysms in patients with chronic pancreatitis. World J Surg. 2007. 31:504–510.19. Francisco LE, Asunción LC, Antonio CA, Ricardo RC, Manuel RP, Caridad MH. Post-traumatic hepatic artery pseudoaneurysm treated with endovascular embolization and thrombin injection. World J Hepatol. 2010. 2:87–90.20. Dambrin C, Marcheix B, Birsan T, Cron C, Muscari F, Suc B, et al. Posttraumatic pseudoaneurysm of the hepatic artery: treatment with ultrasound-guided percutaneous transhepatic thrombin injection. J Trauma. 2005. 59:239–242.21. Sparrow P, Asquith J, Chalmers N. Ultrasonic-guided percutaneous injection of pancreatic pseudoaneurysm with thrombin. Cardiovasc Intervent Radiol. 2003. 26:312–315.22. Bender JS, Bouwman DL, Levison MA, Weaver DW. Pseudocysts and pseudoaneurysms: surgical strategy. Pancreas. 1995. 10:143–147.23. Lopera JE. Embolization in trauma: principles and techniques. Semin Intervent Radiol. 2010. 27:14–28.24. Sanada Y, Kondo H, Goshima S, Kanematsu M, Tanaka Y, Tokuyama Y, et al. Liver abscess after common hepatic artery embolization for delayed hemorrhage following pancreaticoduodenectomy: a case report. Case Report Med. 2010. 2010:280430.25. Madoff DC, Denys A, Wallace MJ, Murthy R, Gupta S, Pillsbury EP, et al. Splenic arterial interventions: anatomy, indications, technical considerations, and potential complications. Radiographics. 2005. 25:Suppl 1. S191–S211.
