Etiology, Clinical Features, and Endoscopic Management of Hemobilia: A Retrospective Analysis of 37 Cases
- Affiliations
-
- 1Department of Internal Medicine, CHA Gumi Medical Center, CHA University, Gumi, Korea.
- 2Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea. tnk@med.yu.ac.kr
- KMID: 1364833
- DOI: http://doi.org/10.4166/kjg.2012.59.4.296
Abstract
- BACKGROUND/AIMS
Hemobilia is a rare cause of upper gastrointestinal bleeding. Endoscopic retrograde cholangiopancreaticography (ERCP) is considered to be an excellent diagnostic and treatment modality. Thirty-seven cases of hemobilia with different underlying pathologies were analyzed to illustrate clinical features and to evaluate the role of endoscopic management.
METHODS
A total of 37 patients (26 men and 11 women; mean age, 66.2+/-15.3 years) who were confirmed to have hemobilia by ERCP in a single center from 2000 to 2010 were reviewed retrospectively. Patients with iatrogenic causes of hemobilia were excluded in this study.
RESULTS
The causes of hemobilia were hepatocellular carcinoma in 14, bile duct and gallbladder malignancies in 12, common bile duct stones with cholangitis in 4, acute cholecystitis in 4, and pancreatic cancer in 2 patients. The clinical features of hemobilia were jaundice (89.2%), abdominal pain (78.4%), and melena (13.5%). The cholangiographic findings of hemobilia were amorphous filling defects in 15, tubular filling defects in 6, and cast-like filling defects in 6 patients. Endoscopic management included endoscopic nasobiliary drainage in 26 patients and endoscopic retrograde biliary drainage in 7 patients. Biliary obstruction caused by hemobilia was successfully treated with endoscopic biliary drainages in most cases.
CONCLUSIONS
The most common non-iatrogenic causes of hemobilia were hepatobiliary malignancies, and the majority of patients presented with jaundice and abdominal pain. Endoscopic biliary drainage is recommended as the initial management to control biliary obstruction.
Keyword
MeSH Terms
-
Abdominal Pain/etiology
Adult
Aged
Aged, 80 and over
Bile Duct Neoplasms/complications
Carcinoma, Hepatocellular/complications
Cholangiopancreatography, Endoscopic Retrograde
Cholecystectomy
Cholecystitis/complications
Drainage
Female
Gallstones/complications
Hemobilia/*diagnosis/etiology/therapy
Humans
Jaundice/etiology
Liver Neoplasms/complications
Male
Middle Aged
Pancreatic Neoplasms/complications
Retrospective Studies
Figure
-
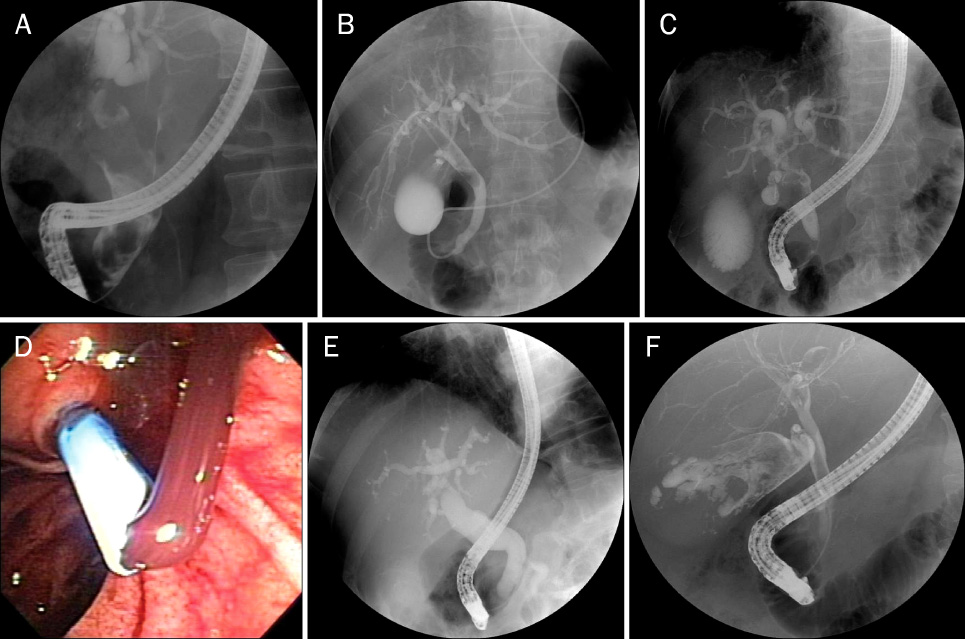
Fig. 1 Endoscopic retrograde cholangiographic findings of hemobilia. (A) In a 59-year-old male with hepatocellular carcinoma, cholangiogram showed a large, cast-like filling defect in the dilated common bile duct. (B) In a 68-year-old male with hepatocellular carcinoma, cholangiogram showed a longitudinal, tubular filling defect in the common bile duct and the right main intrahepatic duct. (C) In a 78-year-old male with common bile duct cancer, cholangiogram showed ill-defined, amorphous filling defects in the proximal common bile duct and bifurcation of the bile duct. (D, E) In a 79-year-old male with acute suppurative cholangitis, ERCP demonstrated that large amounts of blood admixed with pustulous bile was gushing out after endoscopic retrograde biliary drainage, but, cholangiogram showed no demonstrable filling defect in the dilated common bile duct. (F) In a 75-year-old male with gallbladder cancer, cholangiogram showed amorphous filling defects within the distended gallbladder with no demonstrable filling defect in the common bile duct.
Cited by 1 articles
-
Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
Sung Hak Lee, Seung Goun Hong, Kyoung yong Lee, Pyung Kang Park, Sung Du Kim, Mahn Lee, Dong Wook Yu, Man Yong Hong
Clin Endosc. 2016;49(3):303-307. doi: 10.5946/ce.2015.081.
Reference
-
1. Sandblom P. Hemorrhage into the biliary tract following trauma; traumatic hemobilia. Surgery. 1948. 24:571–586.2. Quincke H. Ein fall von aneurysma der leberarterie. Berl Klein Wochenschr. 1871. 30:349–352.3. Alis H, Bozkurt MA, Oner OZ, et al. Case report: acute pancreatitis caused by postcholecystectomic hemobilia. BMC Gastroenterol. 2010. 10:75.4. Park SS, Kim BU, Han HS, et al. Hemobilia from ruptured hepatic artery aneurysm in polyarteritis nodosa. Korean J Intern Med. 2006. 21:79–82.5. Hendriks MP, Wanten GJ, Drenth JP. Management of hemobilia and pancreatitis after liver biopsy: a key role for endoscopic retrograde cholangiopancreaticography. Liver Transpl. 2009. 15:1653–1654.6. Green MH, Duell RM, Johnson CD, Jamieson NV. Haemobilia. Br J Surg. 2001. 88:773–786.7. Yoshida J, Donahue PE, Nyhus LM. Hemobilia: review of recent experience with a worldwide problem. Am J Gastroenterol. 1987. 82:448–453.8. Sandblom P, Mirkovitch V. Minor hemobilia. Clinical significance and pathophysiological background. Ann Surg. 1979. 190:254–264.9. Sandblom P. Hemobilia (Biliary Tract Hemorrhage): History, Diagnosis, and Treatment. 1972. Springfield: Charles C Thomas.10. Chin MW, Enns R. Hemobilia. Curr Gastroenterol Rep. 2010. 12:121–129.11. Bloechle C, Izbicki JR, Rashed MY, et al. Hemobilia: presentation, diagnosis, and management. Am J Gastroenterol. 1994. 89:1537–1540.12. Willemsen PJ, Vanderveken ML, De Caluwe DO, Tielliu IF. Hemobilia: a rare complication of cholecystitis and cholecystolithiasis. Case report. Acta Chir Belg. 1996. 96:93–94.13. Brady E, Welch JP. Acute hemorrhagic cholecystitis causing hemobilia and colonic necrosis. Dis Colon Rectum. 1985. 28:185–187.14. Merrell SW, Schneider PD. Hemobilia-evolution of current diagnosis and treatment. West J Med. 1991. 155:621–625.15. Hasan S, Quintana J, Siddiqui Y, Maldonado V. Carcinoma of the pancreas presenting with hemobilia. Gastrointest Endosc. 1986. 32:305–306.16. Qin LX, Tang ZY. Hepatocellular carcinoma with obstructive jaundice: diagnosis, treatment and prognosis. World J Gastroenterol. 2003. 9:385–391.17. Kojiro M, Kawabata K, Kawano Y, Shirai F, Takemoto N, Nakashima T. Hepatocellular carcinoma presenting as intrabile duct tumor growth: a clinicopathologic study of 24 cases. Cancer. 1982. 49:2144–2147.18. Sax SL, Athey PA, Lamki N, Cadavid GA. Sonographic findings in traumatic hemobilia: report of two cases and review of the literature. J Clin Ultrasound. 1988. 16:29–34.19. Kroser J, Rothstein RD, Kochman ML. Endoscopic management of obstructive jaundice caused by hemobilia. Gastrointest Endosc. 1996. 44:618–619.20. Sandblom P, Mirkovitch V, Saegesser F. Formation and fate of fibrin clots in the biliary tract: a clinical and experimental study. Ann Surg. 1977. 185:356–366.21. Sandblom P, Saegesser F, Mirkovitch V. Hepatic hemobilia: hemorrhage from the intrahepatic biliary tract, a review. World J Surg. 1984. 8:41–50.22. Luzuy F, Reinberg O, Kauszlaric D, et al. Biliary calculi caused by hemobilia. Surgery. 1987. 102:886–889.23. Worobetz LJ, Passi RB, Sullivan SN. Hemobilia after percutaneous liver biopsy: role of endoscopic retrograde cholangiopancreatography and sphincterotomy. Am J Gastroenterol. 1983. 78:182–184.24. Jensen AR, Matzen P. Hemobilia with jaundice: treatment by endoscopic papillotomy. Am J Gastroenterol. 1982. 77:162–163.25. Lee SL, Caruso DM. Acute cholecystitis secondary to hemobilia. J Laparoendosc Adv Surg Tech A. 1999. 9:347–349.26. Baker AR, Corlett SK, Cookson JB, Carr-Locke DL. Hemobilia treated by nasobiliary catheterization. Am J Gastroenterol. 1987. 82:783–785.27. Srivastava DN, Sharma S, Pal S, et al. Transcatheter arterial embolization in the management of hemobilia. Abdom Imaging. 2006. 31:439–448.28. Goodnight JE Jr, Blaisdell FW. Hemobilia. Surg Clin North Am. 1981. 61:973–979.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two cases of gallbladder cancer diagnosed by detection of hemobilia
- Portal cavernography during endoscopic retrograde cholangiopancreatography: from bilhemia to hemobilia
- Two Cases of Hemobilia Associated with Common Bile Duct Stones
- Delayed Severe Hemobilia after Endoscopic Biliary Plastic Stent Insertion
- A case of hemocholecyst associated with hemobilia following radiofrequency ablation therapy for hepatocellular carcinoma
