J Breast Cancer.
2011 Feb;14(Suppl 1):S37-S43. 10.4048/jbc.2011.14.S.S37.
Optimal Sampling Number of Sentinel Lymph Nodes in Invasive Breast Cancer: Results of 1,026 Sentinel Lymph Node Biopsies Done by Radioisotope
- Affiliations
-
- 1Department of Surgery, Yeungnam University College of Medicine, Daegu, Korea. crystallee@med.yu.ac.kr
- 2Department of Pathology, Yeungnam University College of Medicine, Daegu, Korea.
- KMID: 1340912
- DOI: http://doi.org/10.4048/jbc.2011.14.S.S37
Abstract
- PURPOSE
For isotope mapping, many authors have defined the sentinel lymph node (SLN) as the one containing isotope counts higher than the axillary background. However, no study has sought to define an optimal guideline, and the number of SLNs needed for precise detection of metastatic SLNs is still a subject of debate. Accordingly, we set out to determine the optimal sampling number of SLNs.
METHODS
Between January 2005 and December 2008, we enrolled 1,026 patients with primary invasive breast cancer. These patients had received sentinel lymph node biopsy (SLNB) using radioisotopes at Yeungnam University Hospital. During SLNB, ex vivo isotope counts were measured for each SLN. And, the number and metastatic status of harvested SLNs were investigated. We defined SLNs as lymph nodes that show an isotope count > or = 10 times that of the axillary background. Each SLN was labeled as S1 (highest isotope count), S2 (second highest), or S3 and so on, in descending isotope-count-order. If an SLN was positive for metastasis, completion axillary lymph node dissection was performed.
RESULTS
The mean age of patients was 48.9 years (ranges, 22-83 years). The mean number of removed SLNs was 2.8 (ranges, 1-11). Of the 1,026 patients enrolled, 311 (30.3%) had SLN metastasis: S1 was positive (S1+) in 258 patients (82.9%), S2 was positive (S1-, S2+) in 40 patients (12.3%), and S3 was positive (S1-, S2-, S3+) in 13 patients (3.9%). There was no metastasis in SLNs defined as S4, S5 and so on. The average number of sampling SLNs until detecting metastasis in S1, S2, and S3 was 1.24 (1-4), 2.45 (2-4), and 3.46 (3-5).
CONCLUSION
During SLNB done using radioisotopes, for accurate axillary lymph node staging, up to the 3rd isotope-count-order of SLNs should be removed. The average number of SLNs needed for detecting metastasis in S3 is four.
MeSH Terms
Figure
-
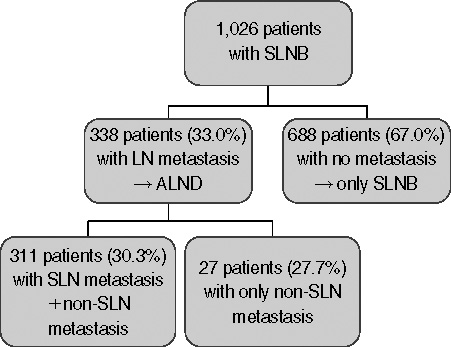
Figure 1 Metastatic status of axillary lymph nodes. SLNB=sentinel lymph node biopsy; ALND=axillary lymph node dissection.
Cited by 1 articles
-
How Many Sentinel Lymph Nodes Are Enough for Accurate Axillary Staging in T1-2 Breast Cancer?
Eun Jeong Ban, Jun Sang Lee, Ja Seung Koo, Seho Park, Seung Il Kim, Byeong-Woo Park
J Breast Cancer. 2011;14(4):296-300. doi: 10.4048/jbc.2011.14.4.296.
Reference
-
1. McMasters KM, Tuttle TM, Carlson DJ, Brown CM, Noyes RD, Glaser RL, et al. Sentinel lymph node biopsy for breast cancer: a suitable alternative to routine axillary dissection in multi-institutional practice when optimal technique is used. J Clin Oncol. 2000. 18:2560–2566.
Article2. Kjaergaard J, Blichert-Toft M, Andersen JA, Rank F, Pedersen BV. Probability of false negative nodal staging in conjunction with partial axillary dissection in breast cancer. Br J Surg. 1985. 72:365–367.
Article3. Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, Storm FK, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992. 127:392–399.
Article4. McCarter MD, Yeung H, Fey J, Borgen PI, Cody HS 3rd. The breast cancer patient with multiple sentinel nodes: when to stop? J Am Coll Surg. 2001. 192:692–697.
Article5. Woznick A, Franco M, Bendick P, Benitez PR. Sentinel lymph node dissection for breast cancer: how many nodes are enough and which technique is optimal? Am J Surg. 2006. 191:330–333.
Article6. Dabbs DJ, Johnson R. The optimal number of sentinel lymph nodes for focused pathologic examination. Breast J. 2004. 10:186–189.
Article7. McLaughlin SA, Wright MJ, Morris KT, Giron GL, Sampson MR, Brockway JP, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol. 2008. 26:5213–5219.
Article8. Fleissig A, Fallowfield LJ, Langridge CI, Johnson L, Newcombe RG, Dixon JM, et al. Post-operative arm morbidity and quality of life. Results of the ALMANAC randomised trial comparing sentinel node biopsy with standard axillary treatment in the management of patients with early breast cancer. Breast Cancer Res Treat. 2006. 95:279–293.
Article9. Hill AD, Tran KN, Akhurst T, Yeung H, Yeh SD, Rosen PP, et al. Lessons learned from 500 cases of lymphatic mapping for breast cancer. Ann Surg. 1999. 229:528–535.
Article10. Cox CE, Pendas S, Cox JM, Joseph E, Shons AR, Yeatman T, et al. Guidelines for sentinel node biopsy and lymphatic mapping of patients with breast cancer. Ann Surg. 1998. 227:645–651.
Article11. Borgstein PJ, Pijpers R, Comans EF, van Diest PJ, Boom RP, Meijer S. Sentinel lymph node biopsy in breast cancer: guidelines and pitfalls of lymphoscintigraphy and gamma probe detection. J Am Coll Surg. 1998. 186:275–283.
Article12. Krag DN, Meijer SJ, Weaver DL, Loggie BW, Harlow SP, Tanabe KK, et al. Minimal-access surgery for staging of malignant melanoma. Arch Surg. 1995. 130:654–658.
Article13. Krag D, Weaver D, Ashikaga T, Moffat F, Klimberg VS, Shriver C, et al. The sentinel node in breast cancer: a multicenter validation study. N Engl J Med. 1998. 339:941–946.
Article14. Schrenk P, Rehberger W, Shamiyeh A, Wayand W. Sentinel node biopsy for breast cancer: does the number of sentinel nodes removed have an impact on the accuracy of finding a positive node? J Surg Oncol. 2002. 80:130–136.
Article15. Yi M, Meric-Bernstam F, Ross MI, Akins JS, Hwang RF, Lucci A, et al. How many sentinel lymph nodes are enough during sentinel lymph node dissection for breast cancer? Cancer. 2008. 113:30–37.
Article16. Koo BY, Jeong SG, Eom TI, Kang HJ, Kim LS. The number of removed lymph nodes for an acceptable false negative rate in sentinel lymph node biopsy for breast cancer. J Breast Cancer. 2009. 12:100–105.
Article17. Martin RC, Fey J, Yeung H, Borgen PI, Cody HS 3rd. Highest isotope count does not predict sentinel node positivity in all breast cancer patients. Ann Surg Oncol. 2001. 8:592–597.
Article18. Baek CS, Park SY, Kang SH, Lee SJ. The classification of sentinel lymph node according to radioactivity in breast cancer. J Korean Surg Soc. 2003. 65:382–388.19. Ollila DW, Brennan MB, Giuliano AE. The role of intraoperative lymphatic mapping and sentinel lymphadenectomy in the management of patients with breast cancer. Adv Surg. 1999. 32:349–364.20. Veronesi U, Paganelli G, Viale G, Galimberti V, Luini A, Zurrida S, et al. Sentinel lymph node biopsy and axillary dissection in breast cancer: results in a large series. J Natl Cancer Inst. 1999. 91:368–373.
Article21. Cody HS 3rd. Sentinel lymph node mapping in breast cancer. Oncology (Williston Park). 1999. 13:25–34.
Article22. Cox CE, Haddad F, Bass S, Cox JM, Ku NN, Berman C, et al. Lymphatic mapping in the treatment of breast cancer. Oncology (Williston Park). 1998. 12:1283–1292.23. McMasters KM, Giuliano AE, Ross MI, Reintgen DS, Hunt KK, Byrd DR, et al. Sentinel-lymph-node biopsy for breast cancer: not yet the standard of care. N Engl J Med. 1998. 339:990–995.
Article24. Nieweg OE, Estourgie SH. What is a sentinel node and what is a false-negative sentinel node? Ann Surg Oncol. 2004. 11:3 Suppl. 169S–173S.
Article25. Nieweg OE. False-negative sentinel node biopsy. Ann Surg Oncol. 2009. 16:2089–2091.
Article26. Hoar FJ, Stonelake PS. A prospective study of the value of axillary node sampling in addition to sentinel lymph node biopsy in patients with breast cancer. Eur J Surg Oncol. 2003. 29:526–531.
Article27. Keskek M, Balas S, Gokoz A, Sayek I. Re-evaluation of axillary skip metastases in the era of sentinel lymph node biopsy in breast cancer. Surg Today. 2006. 36:1047–1052.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Number of Removed Lymph Nodes for an Acceptable False Negative Rate in Sentinel Lymph Node Biopsy for Breast Cancer
- Treatment of Malignant Melanoma Using Sentinel Lymph Node Dissection
- Sentinel Lymph Node Imaging in Breast Cancer
- Optimized Criteria for Sentinel Lymph Node Biopsy in Patients with Clinically Node Negative Breast Cancer
- The Efficacy of Sentinel Lymph Node Biopsy Using Radioisotopes in Breast Cancer Patients
