Pollicization: The Concept, Technical Details, and Outcome
- Affiliations
-
- 1Department of Orthopaedic Surgery, Temple University and Upper Extremity Center of Excellence, Shriners Hospitals for Children, Philadelphia, PA, USA. skozin@shrinenet.org
- KMID: 1245396
- DOI: http://doi.org/10.4055/cios.2012.4.1.18
Abstract
- Pollicization substitutes a functioning finger for a deficient thumb. The most indication is thumb hypoplasia with absence or instability of the carpometacarpal joint. However, there are additional causes that may negate thumb function, such as trauma, macrodactyly, multi-fingered hand, and a mirror hand. The technique of pollicization represents a consolidation of contributions from surgeons over the last 100 years. A meticulous stepwise approach from incision to closure is necessary to optimize outcome. Following pollicization, cortical plasticity and motor relearning play a pivotal role in function following pollicization with connections and adjacent sprouting from nearby cortical and/or subcortical territories. Occupational therapy is necessary to encourage large object acquisition followed by smaller objects and ultimately fine pinch. Pollicization is more reliable in patients with isolated thumb hypoplasia and a mobile index finger with robust extrinsic and intrinsic muscle-tendon units compared to and patients with radial forearm deficiencies and diminished index mobility.
MeSH Terms
Figure
-
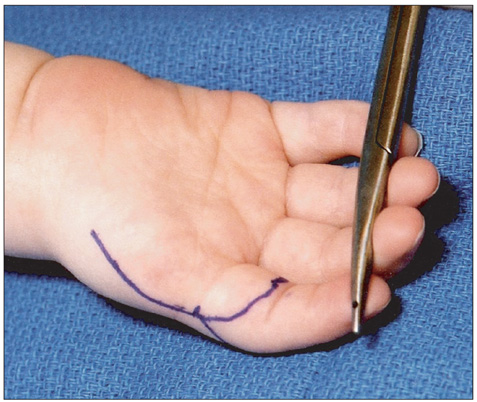
Fig. 1 Volar skin design (Courtesy of Shriners Hospital for Children, Philadelphia).
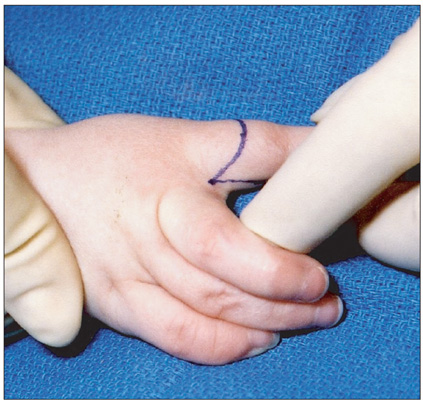
Fig. 2 Dorsal skin design (Courtesy of Shriners Hospital for Children, Philadelphia).
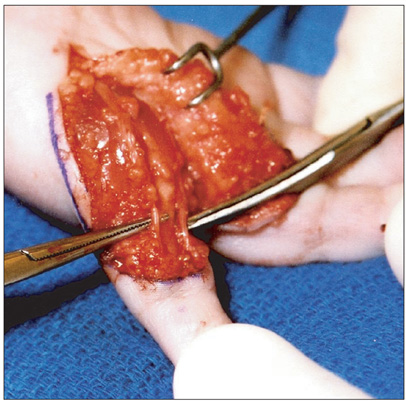
Fig. 3 Isolation of radial and ulnar neurovascular bundles (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 4 Volar dissection of a type IIIB thumb hypoplasia with tracing of the single vessel to radial neurovascular bundle of the index finger (Courtesy of Shriners Hospital for Children, Philadelphia).
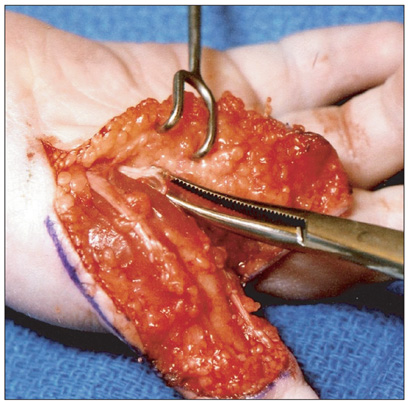
Fig. 5 Microdissection of the common digital nerve between the index and long (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 6 Ligation of the proper digital artery to the long finger (Courtesy of Shriners Hospital for Children, Philadelphia).
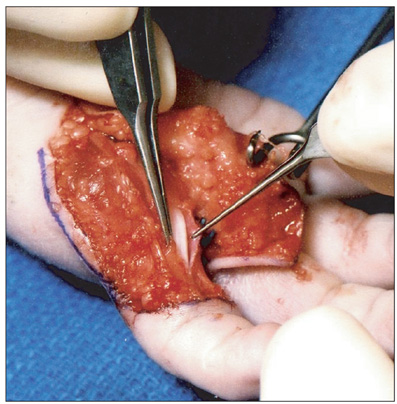
Fig. 7 Incision of the first annular pulley of the index finger (Courtesy of Shriners Hospital for Children, Philadelphia).
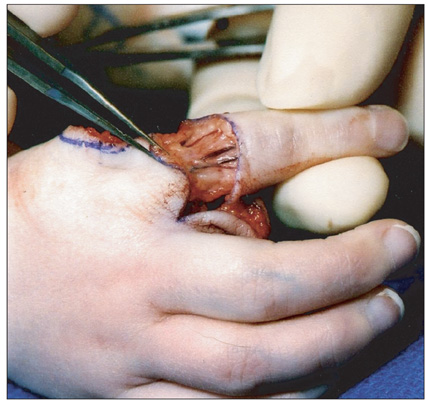
Fig. 8 Elevation of dorsal incision with preservation of dorsal veins (Courtesy of Shriners Hospital for Children, Philadelphia).
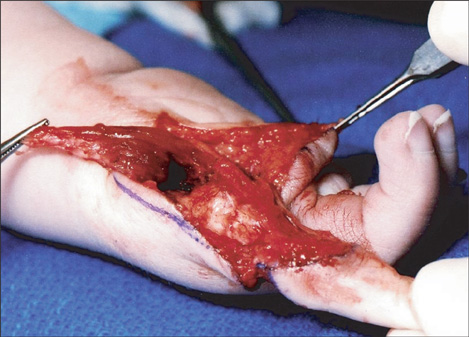
Fig. 9 First dorsal interosseous released from the extensor hood. (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 10 Sutures placed for later transfer of the first dorsal and first palmar interossei (Courtesy of Shriners Hospital for Children, Philadelphia).
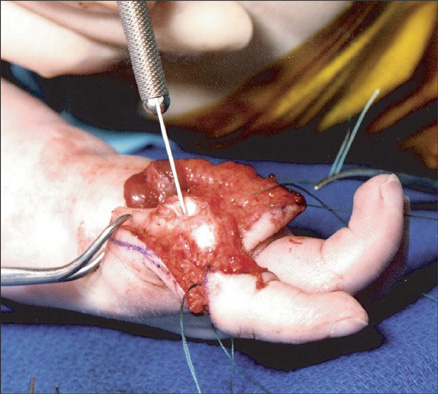
Fig. 11 Distal cut of index metacarpal through the physis (Courtesy of Shriners Hospital for Children, Philadelphia).
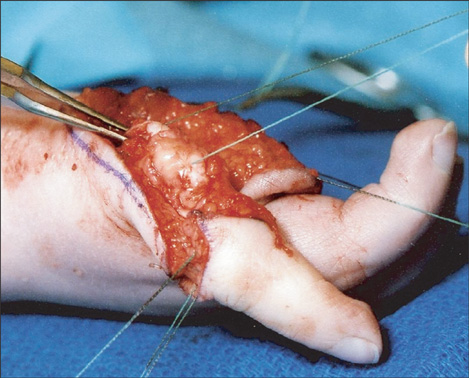
Fig. 12 Metacarpophalangeal joint sutured into hyperextension using a non-absorbable (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 13 Thumb positioned and secured with interosseous sutures (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 14 Intrinsic reconstruction using first dorsal interosseous (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 15 Skin inset and sutured with absorbable suture (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 16 Three-year-old girl with progressive macrodactyly of the left thumb and index digits (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 17 Volar skin design (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 18 Dorsal skin design (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 19 Enlarged median nerve and superficial arch isolated (Courtesy of Shriners Hospital for Children, Philadelphia).
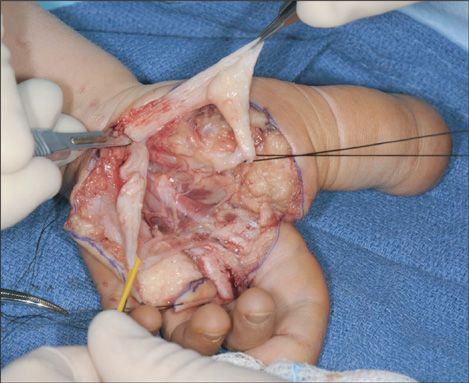
Fig. 20 Digital nerves supplying the long finger are separated from median nerve hamartoma (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 21 Amputation of thumb and index finger with preservation of the index metacarpal (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 22 Long finger metacarpal is removed (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 23 The long finger is inset into the base of the index metacarpal with careful positioning (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 24 Final position after the skin is inset (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 25 Three-year-old girl with bilateral ulnar deficiencies and a left hypoplastic thumb with a bifid metacarpal (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 26 Volar skin incision incorporating thumb ablation (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 27 Dorsal skin incision (Courtesy of Shriners Hospital for Children, Philadelphia).
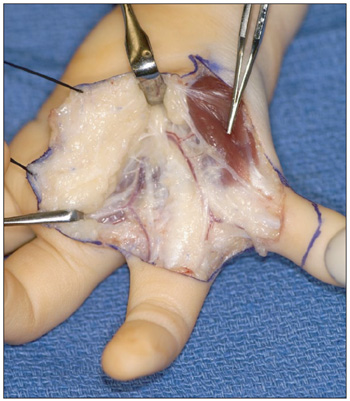
Fig. 28 Isolation of neurovascular bundles and residual abductor pollicis brevis to be incorporated into the pollicization (Courtesy of Shriners Hospital for Children, Philadelphia).
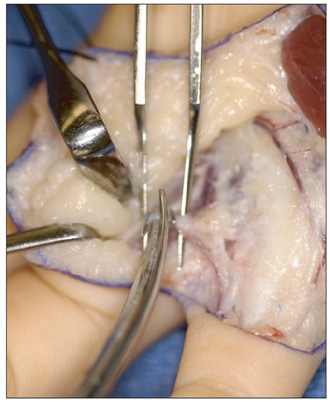
Fig. 29 Ligation of the radial digital artery to the long finger (Courtesy of Shriners Hospital for Children, Philadelphia).
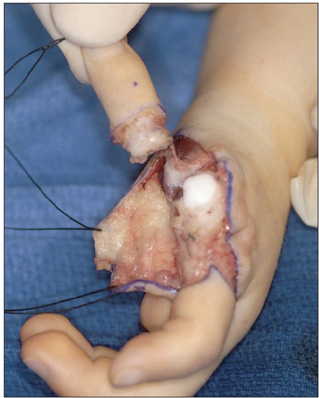
Fig. 30 Amputation of the thumb and its phalanges (Courtesy of Shriners Hospital for Children, Philadelphia).
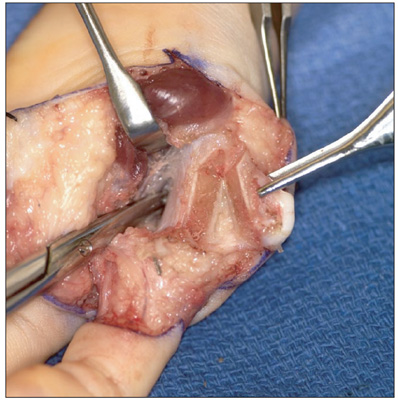
Fig. 31 Resection of the radial portion of the bifid metacarpal with preservation of a large base (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 32 Shortening of the index metacarpal for pollicization (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 33 Fixation with two Kirschner wires and abductor reconstruction (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 34 Skin countering of the first web space (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 35 Closure with 5-0 plain suture (Courtesy of Shriners Hospital for Children, Philadelphia).
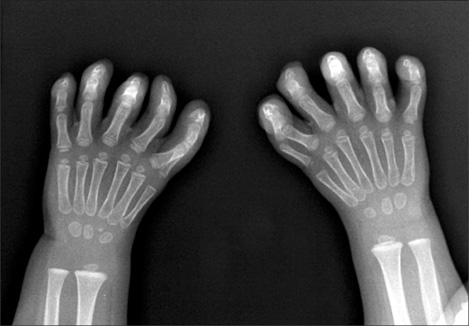
Fig. 36 X-ray of 3-year-old girl with bilateral 6 fingered hands (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 37 Clinical examination demonstrates conjoined motion of the two radial digits (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 38 Volar dissection and identification of neurovascular structures (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 39 Incision of A1 pulleys (Courtesy of Shriners Hospital for Children, Philadelphia).
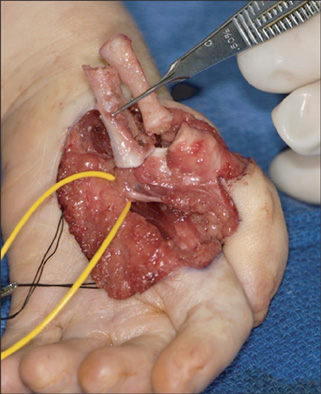
Fig. 40 Excision of both metacarpals (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 41 Postoperative appearance after intrinsic reconstruction and skin closure (Courtesy of Shriners Hospital for Children, Philadelphia).
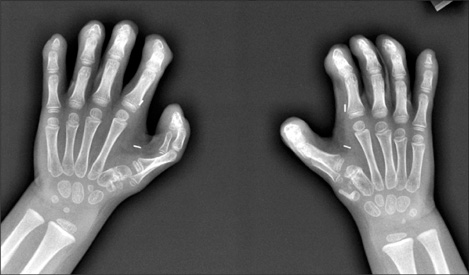
Fig. 42 Subsequent postoperative X-rays following bilateral pollicization (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 43 Left thumb position and pinch function (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 44 Three-year-old girl with mirror hand and seven fingers (Courtesy of Shriners Hospital for Children, Philadelphia).
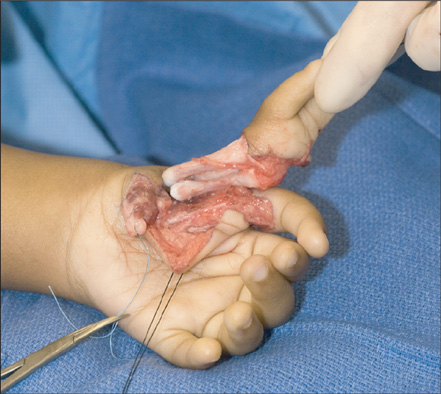
Fig. 45 Ablation of the two less mobile radial digits (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 46 Polllicization of the most mobile radial digit (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 47 Appearance after pollicization (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 48 Activities for encouraging pinch pattern include playing with stickers (Courtesy of Shriners Hospital for Children, Philadelphia).

Fig. 49 Three-year-old with ulnar deficiency depicted in Fig. 25 (Courtesy of Shriners Hospital for Children, Philadelphia). (A) Left thumb position. (B) Gross grasp pattern. (C) Fine pinch pattern.
Reference
-
1. Manske PR, McCaroll HR Jr. Index finger pollicization for a congenitally absent or nonfunctioning thumb. J Hand Surg Am. 1985. 10(5):606–613.
Article2. Kozin SH, Weiss AA, Webber JB, Betz RR, Clancy M, Steel HH. Index finger pollicization for congenital aplasia or hypoplasia of the thumb. J Hand Surg Am. 1992. 17(5):880–884.
Article3. Lister G. Reconstruction of the hypoplastic thumb. Clin Orthop Relat Res. 1985. (195):52–65.
Article4. Foucher G, Medina J, Navarro R. Microsurgical reconstruction of the hypoplastic thumb, type IIIB. J Reconstr Microsurg. 2001. 17(1):9–15.
Article5. Anastakis DJ, Malessy MJ, Chen R, Davis KD, Mikulis D. Cortical plasticity following nerve transfer in the upper extremity. Hand Clin. 2008. 24(4):425–444.
Article6. Chen R. Studies of human motor physiology with transcranial magnetic stimulation. Muscle Nerve Suppl. 2000. 9:S26–S32.
Article7. Barker AT, Jalinous R, Freeston IL. Non-invasive magnetic stimulation of human motor cortex. Lancet. 1985. 1(8437):1106–1107.
Article8. Gevins A, Leong H, Smith ME, Le J, Du R. Mapping cognitive brain function with modern high-resolution electroencephalography. Trends Neurosci. 1995. 18(10):429–436.
Article9. Friston KJ, Frith CD, Liddle PF, Frackowiak RS. Comparing functional (PET) images: the assessment of significant change. J Cereb Blood Flow Metab. 1991. 11(4):690–699.
Article10. Giraux P, Sirigu A, Schneider F, Dubernard JM. Cortical reorganization in motor cortex after graft of both hands. Nat Neurosci. 2001. 4(7):691–692.
Article11. Manduch M, Bezuhly M, Anastakis DJ, Crawley AP, Mikulis DJ. Serial fMRI of adaptive changes in primary sensorimotor cortex following thumb reconstruction. Neurology. 2002. 59(8):1278–1281.
Article12. Chen R, Anastakis DJ, Haywood CT, Mikulis DJ, Manktelow RT. Plasticity of the human motor system following muscle reconstruction: a magnetic stimulation and functional magnetic resonance imaging study. Clin Neurophysiol. 2003. 114(12):2434–2446.
Article13. Buck-Gramcko D. Pollicization of the index finger: method and results in aplasia and hypoplasia of the thumb. J Bone Joint Surg Am. 1971. 53(8):1605–1617.
Article14. Littler JW. On making a thumb: one hundred years of surgical effort. J Hand Surg Am. 1976. 1(1):35–51.
Article15. McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000. 25(6):1007–1037.
Article16. Kozin SH. Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, editors. Deformities of the thumb. Green's operative hand surgery. 2010. 6th ed. Philadelphia, PA: Elsevier Churchill Livingstone;1371–1404.
Article17. Brodwater BK, Major NM, Goldner RD, Layfield LJ. Macrodystrophia lipomatosa with associated fibrolipomatous hamartoma of the median nerve. Pediatr Surg Int. 2000. 16(3):216–218.
Article18. Al-Qattan MM. Lipofibromatous hamartoma of the median nerve and its associated conditions. J Hand Surg Br. 2001. 26(4):368–372.
Article19. Ishida O, Ikuta Y. Long-term results of surgical treatment for macrodactyly of the hand. Plast Reconstr Surg. 1998. 102(5):1586–1590.
Article20. Kozin SH. Upper-extremity congenital anomalies. J Bone Joint Surg Am. 2003. 85(8):1564–1576.
Article21. Cole RJ, Manske PR. Classification of ulnar deficiency according to the thumb and first web. J Hand Surg Am. 1997. 22(3):479–488.22. Al-Qattan MM, Al-Thunayan A, De Cordier M, Nandagopal N, Pitkanen J. Classification of the mirror hand-multiple hand spectrum. J Hand Surg Br. 1998. 23(4):534–536.23. Riddle RD, Johnson RL, Laufer E, Tabin C. Sonic hedgehog mediates the polarizing activity of the ZPA. Cell. 1993. 75(7):1401–1416.24. Barton NJ, Buck-Gramcko D, Evans DM. Soft-tissue anatomy of mirror hand. J Hand Surg Br. 1986. 11(3):307–319.25. Barton NJ, Buck-Gramcko D, Evans DM, Kleinert H, Semple C, Ulson H. Mirror hand treated by true pollicization. J Hand Surg Br. 1986. 11(3):320–336.26. Manske PR, Rotman MB, Dailey LA. Long-term functional results after pollicization for the congenitally deficient thumb. J Hand Surg Am. 1992. 17(6):1064–1072.27. Clark DI, Chell J, Davis TR. Pollicisation of the index finger: a 27-year follow-up study. J Bone Joint Surg Br. 1998. 80(4):631–635.
Article28. Ogino T, Ishii S. Long-term results after pollicization for congenital hand deformities. Hand Surg. 1997. 2(2):79–85.
Article29. Sykes PJ, Chandraprakasam T, Percival NJ. Pollicisation of the index finger in congenital anomalies: a retrospective analysis. J Hand Surg Br. 1991. 16(2):144–147.30. Vekris MD, Beris AE, Lykissas MG, Soucacos PN. Index finger pollicization in the treatment of congenitally deficient thumb. Ann Plast Surg. 2011. 66(2):137–142.31. Ogino T, Minami A, Fukuda K. Abductor digitiminimi opponensplasty in hypoplastic thumb. J Hand Surg Br. 1986. 11(3):372–377.
Article32. Latimer J, Shah M, Kay S. Abductor digitiminimi transfer for the restoration of opposition in children. J Hand Surg Br. 1994. 19(5):653–658.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pollicization of Patients with more than Buck-Gramcko Grade IV Congenital Hypoplasia of the Thumb
- Pollicization of the Middle Finger
- Pollicization: Two Cases report
- Reconstruction of Mutilating Hand with Pollicization and Anteromedial Thigh Perforator Free Flap: A Case Report
- Clinical experiences in Thumb reconstruction
