Early and Delayed Myocardial Enhancement in Myocardial Infarction Using Two-Phase Contrast-Enhanced Multidetector-Row CT
- Affiliations
-
- 1Department of Radiology, University of Keimyung College of Medicine, Dongsan Medical Center, Daegu, Korea. ksm9723@yahoo.co.kr
- 2Department of Internal Medicine, University of Keimyung College of Medicine, Dongsan Medical Center, Daegu, Korea.
- 3Department of Radiology, Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 1126832
- DOI: http://doi.org/10.3348/kjr.2007.8.2.94
Abstract
OBJECTIVE
The purpose of this study was to describe the myocardial enhancement patterns in patients with myocardial infarction using two-phase contrast-enhanced multidetector-row computed tomography (MDCT). MATERIALS AND METHODS: Twenty-three patients with clinically proven myocardial infarction (17 acute myocardial infarction [AMI] and 6 chronic myocardial infarction [CMI]) were examined with two-phase contrast-enhanced ECG-gated MDCT. The presence, location, and patterns of myocardial enhancement on two-phase MDCT images were compared with infarcted myocardial territories determined by using electrocardiogram, echocardiography, thallium-201 single photon emission computed tomography, catheter and MDCT coronary angiography. RESULTS: After clinical assessment, the presence of myocardial infarctions were found in 27 territories (19 AMI and 8 CMI) of 23 patients. Early perfusion defects were observed in 30 territories of all 23 patients. Three territories not corresponding to a myocardial infarction were detected in three patients with AMI and were associated with artifacts. Fourteen of perfusion defects were in the left anterior descending artery territory, four in the left circumflex artery territory, and nine in the right coronary artery territory. Delayed enhancement was observed in 25 territories (17 AMI and 8 CMI) of 21 patients. Delayed enhancement patterns were variable. Transmural early perfusion defects (n =12) were closely associated with transmural late enhancement (n = 5) and subendocardial residual defect with subepicardial late enhancement (n = 5). CONCLUSION: Myocardial infarction showed early perfusion defects and variable delayed enhancement patterns on two-phase contrast-enhanced MDCT. Delayed enhancement technique of MDCT could provide additional information of the location and extent of infarcted myocardium, and could be useful to plan appropriate therapeutic strategies in patients with AMI.
Keyword
MeSH Terms
Figure
-
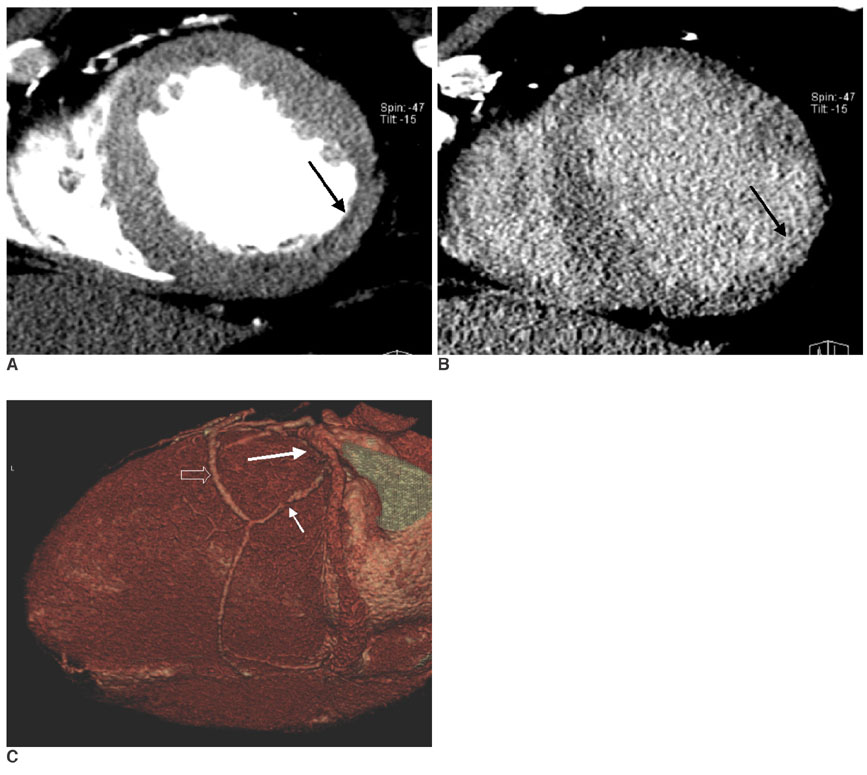
Fig. 1 Images obtained in a 57-year-old man with chronic myocardial infarction. A. The short-axis multiplanar reformation image obtained with early-phase multidetector CT shows a subendocardial hypoenhancement involving the mid-inferolateral myocardium with mild wall thinning (arrow), which corresponds to chronic myocardial infarction of the left circumflex coronary artery territory. B. The short-axis multiplanar reformation image obtained with late-phase multidetector CT shows subendocardial late enhancement in the same area (arrow). C. The volume rendered image shows occlusion of the left circumflex artery (large arrow) and significant stenosis of the obtuse marginal artery (small arrow). A T-graft with the radial artery (open arrow) from the left internal mammary artery to the obtuse marginal artery and the distal anastomosis are open.

Fig. 2 Images obtained in a 73-year-old man with reperfused acute myocardial infarction. A. The short-axis multiplanar reformation image obtained with early-phase multidetector CT shows an early perfusion defect involving the whole thickness of the mid-anterolateral myocardium (arrow), which corresponds to significant stenosis of the left circumflex coronary artery. B. The short-axis multiplanar reformation image obtained with late-phase multidetector CT shows transmural late enhancement in the same area (arrow). Note the total absence of residual perfusion defect within the hyperenhanced area. C. Right oblique caudal projection of the left coronary angiogram shows total occlusion with bridge collateral flow at the proximal segment of the left circumflex coronary artery (arrow).

Fig. 3 Images obtained in a 72-year-old man with reperfused acute myocardial infarction. A. The short-axis multiplanar reformation image obtained with early phase multidetector CT shows a transmural perfusion defect involving the mid-inferior myocardium (arrow), and this corresponds to significant stenosis of the right coronary artery. B. The short-axis multiplanar reformation image obtained with late phase multidetector CT shows subendocardial residual perfusion defect (arrow) with subepicardial late enhancement (arrowhead) in the same area. C. The left oblique projection of the right coronary angiogram shows multiple stenoses in the proximal and middle (arrows) right coronary artery and total occlusion at the distal segment (arrowhead) of the right coronary artery.
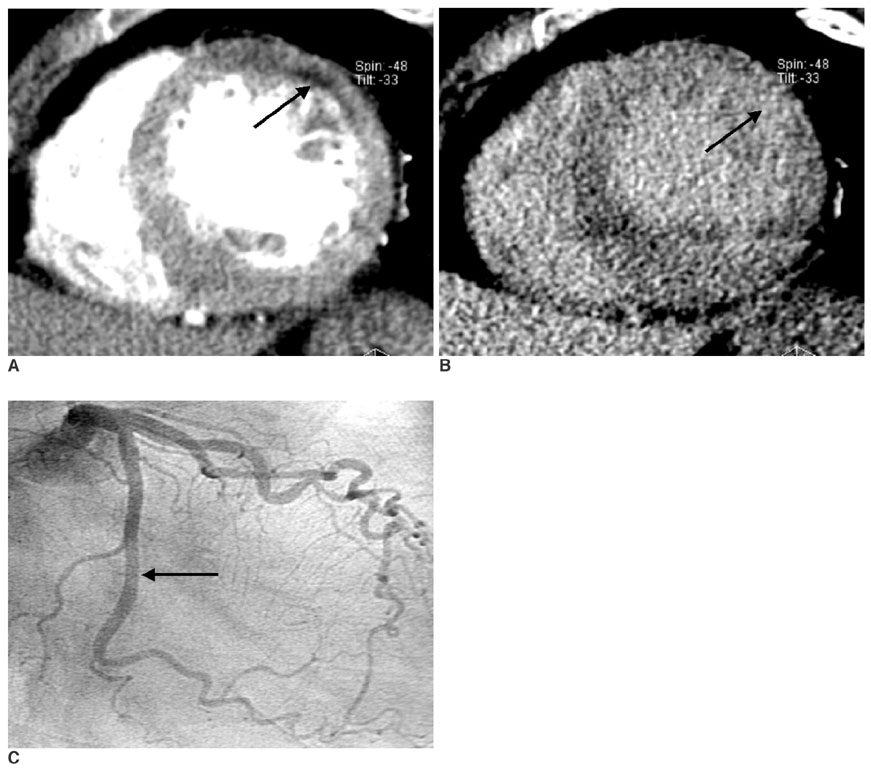
Fig. 4 The images obtained in a 63-year-old woman with reperfused acute myocardial infarction. A. The short-axis multiplanar reformation image obtained with early phase multidetector CT shows a subendocardial perfusion defect involving the mid-anterior and anterolateral myocardium (arrow), and this corresponds to significant stenosis of the left circumflex coronary artery. B. The short-axis multiplanar reformation image obtained with late phase multidetector CT shows transmural late enhancement in the same area (arrow). C. The right anterior oblique caudal projection of the left coronary angiogram shows minimal lesion at the middle segment of the left circumflex coronary artery (arrow).
Cited by 4 articles
-
Role of Cardiac Computed Tomography in the Diagnosis of Left Ventricular Myocardial Diseases
Sung Min Ko, Sung Ho Hwang, Hye-Jeong Lee
J Cardiovasc Imaging. 2019;27(2):73-92. doi: 10.4250/jcvi.2019.27.e17.Assessment of Left Ventricular Myocardial Diseases with Cardiac Computed Tomography
Sung Min Ko, Tae Hoon Kim, Eun Ju Chun, Jin Young Kim, Sung Ho Hwang
Korean J Radiol. 2019;20(3):333-351. doi: 10.3348/kjr.2018.0280.Myocardial Contractility, Perfusion, and Viability Analysis Using Multidetector CT in Patients with Ischemic Heart Disease
Sung Min Ko
J Korean Med Assoc. 2007;50(2):143-150. doi: 10.5124/jkma.2007.50.2.143.Time Efficiency and Diagnostic Accuracy of New Automated Myocardial Perfusion Analysis Software in 320-Row CT Cardiac Imaging
Matthias Rief, Fabian Stenzel, Anisha Kranz, Peter Schlattmann, Marc Dewey
Korean J Radiol. 2013;14(1):21-29. doi: 10.3348/kjr.2013.14.1.21.
Reference
-
1. Kloner RA, Jennings RB. Consequences of brief ischemia: stunning, preconditioning, and their clinical implications: part 1. Circulation. 2001. 104:2981–2989.2. Sandstede JJ. Assessment of myocardial viability by MR imaging. Eur Radiol. 2003. 13:52–61.3. Richard V, Murry CE, Reimer KA. Healing of myocardial infarcts in dogs: effects of late reperfusion. Circulation. 1995. 92:1891–1901.4. Lipton MJ, Higgins CB. Evaluation of ischemic heart disease by computerized transmission tomography. Radiol Clin North Am. 1980. 18:557–576.5. Godwin JD, Moore AV, Ideker RE, Califf RM. Prospective demonstration of myocardial infarction by CT. AJR Am J Roentgenol. 1984. 143:985–986.6. Kramer PH, Goldstein JA, Herkens RJ, Lipton MJ, Brundage BH. Imaging of acute myocardial infarction in man with contrast-enhanced computed transmission tomography. Am Heart J. 1984. 108:1514–1523.7. Nieman K, Cademartiri F, Lemos PA, Raaijmarkers R, Pattynama PM, de Feyter PJ. Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography. Circulation. 2002. 106:2051–2054.8. Ropers D, Baum U, Pohle K, Anders K, Ulzheimer S, Ohnesorge B, et al. Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstruction. Circulation. 2003. 107:664–666.9. Nieman K, Oudkerk M, Rensing BJ, van Ooijen P, Munne A, van Geuns RJ, et al. Coronary angiography with multi-slice computed tomography. Lancet. 2001. 357:599–603.10. Juergens KU, Grude M, Fallenberg EM, Opitz C, Wichter T, Heindel W, et al. Using ECG-gated multidetector CT to evaluate global left ventricular myocardial function in patients with coronary artery disease. AJR Am J Roentgenol. 2002. 179:1545–1550.11. Park JM, Choe YH, Chang S, Sung YM, Kang SS, Kim MJ, et al. Usefulness of multidetector-row CT in the evaluation of reperfused myocardial infarction in a rabbit model. Korean J Radiol. 2004. 5:19–24.12. Nikolaou K, Knez A, Sagmeister S, Wintersperger BJ, Boekstegers P, Steinbeck G, et al. Assessment of myocardial infarctions using multidetector-row computed tomography. J Comput Assist Tomogr. 2004. 28:286–292.13. Nikolaou K, Sanz J, Poon M, Wintersperger BJ, Ohnesorge B, Rius T, et al. Assessment of myocardial perfusion and viability from routine contrast-enhanced 16-detector-row computed tomography of the heart: preliminary results. Eur Radiol. 2005. 15:864–871.14. Koyama Y, Mochizuki T, Higaki J. Computed tomography assessment of myocardial perfusion, viability, and function. J Magn Reson Imaging. 2004. 19:800–815.15. Koyama Y, Matsuoka H, Mochizuki T, Higashino H, Kawakami H, Nakata S, et al. Assessment of reperfused acute myocardial infarction with two-phase contrast-enhanced helical CT: prediction of left ventricular function and wall thickness. Radiology. 2005. 235:804–811.16. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002. 105:539–542.17. Gould RG. Perfusion quantitation by ultrafast computed tomography. Invest Radiol. 1992. 27:Suppl 2. S18–S21.18. Budoff MJ, Georgiou D, Brody A, Agatston AS, Kennedy J, Wolfkiel C, et al. Ultrafast computed tomography as a diagnostic modality in the detection of coronary artery disease: a multicenter study. Circulation. 1996. 93:898–904.19. Knollmann FD, Muschick P, Krause W, Hausmann H, Hetzer R, Felix R. Detection of myocardial ischemia by electron beam CT. Acta Radiol. 2001. 42:386–392.20. Kim RJ, Chen EL, Lima JA, Judd RM. Myocardial Gd-DTPA kinetics determine MRI contrast enhancement and reflect the extent and severity of myocardial injury after acute reperfused infarction. Circulation. 1996. 94:3318–3326.21. Fieno DS, Kim RJ, Chen EL, Lomasney JW, Klocke FJ, Judd RM. Contrast-enhanced magnetic resonance imaging of myocardium at risk: distinction between reversible and irreversible injury throughout infarct healing. J Am Coll Cardiol. 2000. 36:1985–1991.22. Rogers WJ Jr, Kramer CM, Geskin G, Hu YL, Theobald TM, Vido DA, et al. Early contrast-enhanced MRI predicts late functional recovery after reperfused myocardial infarction. Circulation. 1999. 99:744–750.23. Poon M, Fuster V, Fayad Z. Cardiac magnetic resonance imaging: a "one-stop-shop" evaluation of myocardial dysfunction. Curr Opin Cardiol. 2002. 17:663–670.24. Sandstede JJ, Lipke C, Beer M, Harre K, Pabst T, Kenn W, et al. Analysis of first-pass and delayed contrast-enhancement patterns of dysfunctional myocardium on MR imaging: use in the prediction of myocardial viability. AJR Am J Roentgenol. 2000. 174:1737–1740.25. Gould KL, Lipscomb K. Effects of coronary stenoses on coronary flow reserve and resistance. Am J Cardiol. 1974. 34:48–55.26. Kurata A, Mochizuki T, Koyama Y, Haraikawa T, Suzuki J, Shigematsu Y, et al. Myocardial perfusion imaging using adenosine triphosphate stress multi-slice spiral computed tomography: alternative to stress myocardial perfusion scintigraphy. Circ J. 2005. 69:550–557.27. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000. 343:1445–1453.28. Shan K, Constantine G, Sivananthan M, Flamm SD. Role of cardiac magnetic resonance imaging in the assessment of myocardial viability. Circulation. 2004. 109:1328–1334.29. Paul JF, Wartski M, Caussin C, Sigal-Cinqualbre A, Lancelin B, Angel C, et al. Late defect on delayed contrast-enhanced multi-detector row CT scans in the prediction of SPECT infarct size after reperfused acute myocardial infarction: initial experience. Radiology. 2005. 236:485–489.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Multidetector-row CT in the Evaluation of Reperfused Myocardial Infarction in a Rabbit Model
- Usefulness of Contrast-Enhanced Magnetic Resonance Imaging in the Prediction of Myocardial Viability after Acute Myocardial Infarction
- Occlusive Acute Myocardial Infarct on 16 Multidetector-row Helical CT: An Experimental Study in Rabbits
- Evaluation of Reperfused Myocardial Infarction by Low-Dose Multidetector Computed Tomography Using Prospective Electrocardiography (ECG)-Triggering: Comparison with Magnetic Resonance Imaging
- Serum Myoglobin in the Early Phase of Acute Myocardial Infarction
