Clin Orthop Surg.
2009 Jun;1(2):110-113. 10.4055/cios.2009.1.2.110.
Utility of Preoperative Distractive Stress Radiograph for Beginners to Extent of Medial Release in Total Knee Arthroplasty
- Affiliations
-
- 1Department of Orthopaedic Surgery, Gil Medical Center, Gachon University, Incheon, Korea. bklee@gilhospital.com
- KMID: 1122641
- DOI: http://doi.org/10.4055/cios.2009.1.2.110
Abstract
-
BACKGROUND: This study evaluated the preoperative distractive stress radiographs in order to quantify and predict the extent of medial release according to the degree of varus deformity in primary total knee arthroplasty.
METHODS
We evaluated 120 varus, osteoarthritic knee joints (75 patients). The association of the angle on the distractive stress radiograph with extent of medial release was analyzed. The extent of medial release was classified into the following 4 groups according to the stage: release of the deep medial collateral ligament (group 1), release of the posterior oblique ligament and/or semimembranous tendon (group 2), release of the posterior capsule (group 3) and release of the superficial medial collateral ligament (group 4).
RESULTS
The mean femorotibial angle on the preoperative distractive stress radiograph was valgus 2.4degrees (group 1), valgus 0.8degrees (group 2), varus 2.1degrees (group 3) and varus 2.7degrees (group 4). The extent of medial release increased with increasing degree of varus deformity seen on the preoperative distractive stress radiograph.
CONCLUSIONS
The preoperative distractive stress radiograph was useful for predicting the extent of medial release when performing primary total knee arthroplaty.
MeSH Terms
Figure
-
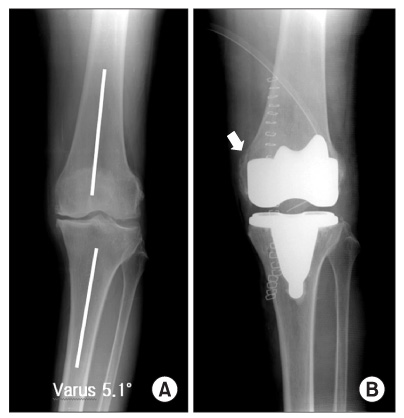
Fig. 1 The femorotibial angle on the preoperative distractive stress radiograph showed varus 5.1° (A). Stage IV release with a medial epicondylar osteotomy was needed for proper ligament balance (B).
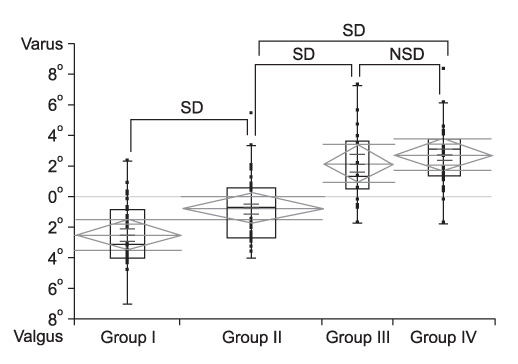
Fig. 2 The femorotibial angles on the preoperative distractive stress radiograph. SD: Significant difference, NSD: No significant difference.
Cited by 1 articles
-
Quantification of the Effect of Vertical Bone Resection of the Medial Proximal Tibia for Achieving Soft Tissue Balancing in Total Knee Arthroplasty
Ji Hyun Ahn, Sung Hyun Lee, Ho Won Kang
Clin Orthop Surg. 2016;8(1):49-56. doi: 10.4055/cios.2016.8.1.49.
Reference
-
1. Engh GA, Ammeen D. Results of total knee arthroplasty with medial epicondylar osteotomy to correct varus deformity. Clin Orthop Relat Res. 1999. (367):141–148.
Article2. Bottros J, Gad B, Krebs V, Barsoum WK. Gap balancing in total knee arthroplasty. J Arthroplasty. 2006. 21(4):Suppl 1. 11–15.
Article3. Mihalko WM, Krackow KA. Flexion and extension gap balancing in revision total knee arthroplasty. Clin Orthop Relat Res. 2006. (446):121–126.
Article4. Yagishita K, Muneta T, Ikeda H. Step-by-step measurements of soft tissue balancing during total knee arthroplasty for patients with varus knees. J Arthroplasty. 2003. 18(3):313–320.
Article5. Matsueda M, Gengerke TR, Murphy M, Lew WD, Gustilo RB. Soft tissue release in total knee arthroplasty: cadaver study using knees without deformities. Clin Orthop Relat Res. 1999. (366):264–273.6. Griffin FM, Insall JN, Scuderi GR. Accuracy of soft tissue balancing in total knee arthroplasty. J Arthroplasty. 2000. 15(8):970–973.
Article7. Clayton ML, Thompson TR, Mack RP. Correction of alignment deformities during total knee arthroplasties: staged soft-tissue releases. Clin Orthop Relat Res. 1986. (202):117–124.8. Luring C, Hufner T, Perlick L, Bathis H, Krettek C, Grifka J. The effectiveness of sequential medial soft tissue release on coronal alignment in total knee arthroplasty: using a computer navigation model. J Arthroplasty. 2006. 21(3):428–434.
Article9. Freeman MA, Todd RC, Bamert P, Day WH. ICLH arthroplasty of the knee: 1968-1977. J Bone Joint Surg Br. 1978. 60(3):339–344.
Article10. Insall JN, Binazzi R, Soudry M, Mestriner LA. Total knee arthroplasty. Clin Orthop Relat Res. 1985. (192):13–22.
Article11. Mihalko WM, Whiteside LA, Krackow KA. Comparison of ligament-balancing techniques during total knee arthroplasty. J Bone Joint Surg Am. 2003. 85:Suppl 4. 132–135.
Article12. Whiteside LA, Saeki K, Mihalko WM. Functional medical ligament balancing in total knee arthroplasty. Clin Orthop Relat Res. 2000. (380):45–57.13. Patel DV, Ferris BD, Aichroth PM. Radiological study of alignment after total knee replacement: short radiographs or long radiographs? Int Orthop. 1991. 15(3):209–210.14. Petersen TL, Engh GA. Radiographic assessment of knee alignment after total knee arthroplasty. J Arthroplasty. 1988. 3(1):67–72.
Article15. Teter KE, Bregman D, Colwell CW Jr. The efficacy of intramedullary femoral alignment in total knee replacement. Clin Orthop Relat Res. 1995. (321):117–121.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship between Tibial Bone Defect and Extent of Medial Release in Total Knee Arthroplasty
- Preoperative Varus-Valgus Stress Angle Difference Is Valuable for Predicting the Extent of Medial Release in Varus Deformity during Total Knee Arthroplasty
- Comparison of Complete Distal Release of the Medial Collateral Ligament and Medial Epicondylar Osteotomy during Ligament Balancing in Varus Knee Total Knee Arthroplasty
- A Novel Medial Soft Tissue Release Method for Varus Deformity during Total Knee Arthroplasty: Femoral Origin Release of the Medial Collateral Ligament
- Lateral Retinacular Release in Total Knee Arthroplasty; Patella Resurfacing versus Retaining
